While we’re pouring resources into learning what keeps cancer cells alive, with the aim of blocking their supply lines, there is next to no interest in the molecular pathways that end up choking the life out of cancer patients, or in the biology behind the longer and better lives that palliative care can offer. Janet Fricker talks to some lone voices about why this has to change.
While death itself may always represent the Great Unknown, the biological processes that contribute to making life no longer viable should be amenable to exploration, yet we know very little about them.
Whether dying from cancer, or other conditions like heart failure or chronic obstructive pulmonary disease, a limited field of research suggests there are integrated biochemical systems that result in a final common pathway, leading to the body shutting down and death. But little is understood about the underlying components of these pathways and how they interconnect.
“It’s extraordinary that in over 5,000 years of medicine, the only thing we really know about death is how to describe it,” says Seamus Coyle, a palliative care consultant from the University of Liverpool, UK, who is one of the few investigators undertaking research into the biological processes of death. “The reality is that the fundamental biology of how people actually die represents a complete black hole.”
The deficit of knowledge around the science of death was highlighted by Julia Neuberger in her 2013 review of the Liverpool Care Pathway, ‘More Care Less Pathway’. In the review, Neuberger commented that there was no precise scientific way of telling accurately when a patient was in their last few days of life. Her recommendations, which have gone largely unheeded, were for the need to boost research into the biology of dying.
Greater understanding of the biological foundation of death would shed light on patterns of death and identify new approaches for palliating distressing symptoms. It would also introduce more certainty about how long people have to live, allowing them, their families, and their doctors to better manage their final months, weeks and days of life, and help to prevent futile anticancer treatments that are all too often given to dying patients.
“The fundamental biology of how people actually die represents a complete black hole”
Such knowledge might also help inform how we care for our patients in what has been described as the ‘grey zone’ – the space occupied by long-term survivors of cancer with metastatic disease. Identifying the final pathways could result in new avenues of treatment targeting the molecular events underlying the lethal biology. Having a scientific foundation for understanding the processes of death would also better inform legal and ethical issues at the end of life, such as assisted suicide.
“By understanding so little about the biology of death we don’t know how to optimally care for terminally ill patients,” says Irene Higginson, a palliative care consultant who directs the Cicely Saunders Institute at King’s College, London. The lack of knowledge, she adds, means that we are in effect abandoning the 1.3 million people who die from cancer in Europe each year.
While there is cause for celebration around recent advances in cancer treatments, a statistic that is conveniently forgotten is that 40% of people diagnosed with cancer ultimately die from the disease. Today, the dying are like new world explorers navigating uncharted waters, with much of their care based on the clinical intuition of palliative specialists rather than having a solid evidence base in rigorous clinical trials. A study undertaken at MD Anderson Cancer Center, Houston, Texas, for example, found that one third of prescriptions given to cancer patients in an acute palliative setting were off-label, signifying the lack of FDA-approved medications for symptom control (J Pain Symptom Manage 2017, 54:46–54).
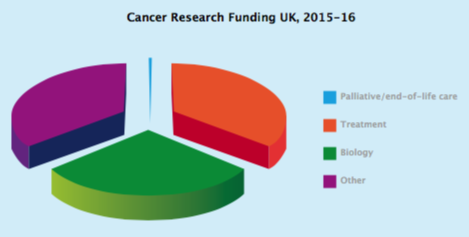
Underpinning the paucity of end-of-life research is the disproportionate amount of research funding spent on oncology versus palliative care. Data by National Cancer Research Institute partners in the UK for 2015–16 found that, of the almost £ 580 million (circa ÿ 630 million) awarded for cancer research, only 0.33% (less than £ 2 million) was allocated to palliative and end-of-life care (ncri.org.uk/ncri-cancer-researchdatabase, accessed on 14 August, 2018, cited in the Lancet Oncol 2018, 19: e588–653).
A similar landscape emerges in the US, with statistics from 2010 showing that palliative care research accounted for only 1% of the National Cancer Institute’s $ 5 billion research funding.
The pathways leading to death attract almost no research funding
Forty per cent of patients diagnosed with cancer go on to die from the disease. Yet gures from the UK for 2015-16 show research into palliative/end-of-life care received 0.33% of the £580 million (circa €630 million) total funding for cancer research, and only a small proportion of that goes towards understanding the biology.
US gures show a similar picture, with only 1% of the National Cancer Institute’s total appropriation for 2010 of US$ 5 billion being awarded to palliative care research (Lancet 2012, 379:519).
Charities, such as Cancer Research UK, for example, have taken strategic decisions not to fund palliative or end-of-life care, and have instead focused on the zeitgeist of precision anticancer medicine. And while the European Commission made EU money available for palliative care research in their Health, Demographic Change and Wellbeing Work Programme, with the 2017 Horizon 2020 call for ‘novel patient-centred approaches for survivorship, palliation and/or end-of-life care’, most of the funding was awarded to organisational work, such as service delivery. “There has been altogether less emphasis on the biology of cancer death, symptom management and how patients live with their cancer,” says Stein Kaasa, who heads the European Palliative Care Research Centre at the University of Oslo, Norway.
Good palliative care prolongs life
“End-of-life research has undoubtedly been the victim of oncology’s recent successes in targeted, immune and proton therapies,” says Kaasa. “There’s been a societal shift where the public thinks it’s now possible to cure most cancers.” With all the hype surrounding drugs, he adds, it can be all too easy to lose sight of the fact that good palliative care prolongs life.
Evidence for the efficacy of palliative care comes from a landmark study by Jennifer Temel, from Massachusetts General Hospital, in Boston, where 151 patients with metastatic lung cancer were randomised to receive early palliative care and standard oncology treatment or standard oncology treatment alone (NEJM 2010, 363:733–42). The study found that patients who received early palliative care not only experienced a better quality of life, reduced burden of symptoms, and less depression, but their median survival time was also longer (11.6 months for those receiving palliative care versus 8.9 months for standard oncology treatment, P=0.02).
Cytokine over-production activates multiple clinical pathways that result in conditions such as cachexia and hypercoagulability
A second study, undertaken at Memorial Sloan Kettering Cancer Center, New York, randomised 766 patients starting routine chemotherapy for metastatic solid tumours to usual care or electronic patient-reported outcomes (PROs), where subjects reported 12 common symptoms to a web-based platform, triggering email alerts to nurses responsible for their care (JAMA 2017, 318:197–98). Results showed that median overall survival was 31.2 months in the PRO group versus 26 months in the usual care group (P=0.03).
“The effect sizes of good palliative care of two to five months are comparable to some of the new therapies for lung cancer. But they’ve additional benefits of having no side effects and being remarkably cost effective,” says Kaasa, who works as both an oncologist and palliative care consultant.
Biological mechanisms of palliative care
One theory of what lies behind the beneficial effects of palliative care is that it could be exerting a fundamental influence on the biochemical processes involved in the final common death pathway. “By supporting patients with palliative care and making them feel less stressed we might be beneficially influencing cytokine levels in their body,” suggests Higginson, who recently failed to secure funding for a study quantifying the effects of palliative care on patient cytokine levels.
Over production of cytokines, says Kenneth Pienta, from John Hopkins University, in Baltimore, Maryland, represents one of the three main clinical categories responsible for death in cancer patients. The other categories are death due to specific organ failure (as occurs, for instance, in patients with brain or liver metastases) and opioid-induced comas that can result in patients with bone metastases requiring higher and higher doses of opioids (as can occur in prostate and breast cancer). In a review written back in 2007, entitled ‘The Lethal Phenotype of Cancer: the Molecular Basis of Death Due to Malignancy’, Pienta wrote that cytokine overproduction activates multiple clinical pathways that result in conditions such as cachexia, which he estimated to be responsible for 20% of cancer deaths, and hypercoagulability, which he estimated to be responsible for 10% of cancer deaths, including those from pulmonary embolism (CA Cancer J Clin 2007, 57:225–41).
The concept of a ‘terminal cancer syndrome’ was described in a 1988 paper outlining how patients with all types of advanced cancer are affected by similar systemic manifestations, including changes in appetite, disturbed sleep, low mood, fatigue, asthenia (loss of strength) and hypercoagulability, which occur regardless of the primary or metastatic site (Arch Intern Med 1988, 148:1586–91). This final common pathway, Pienta believes, is mediated by cytokines.
In his review Pienta describes studies that he undertook showing that cytokines, including tumour necrosis factor-α (TNF-α), interleukin-1 (IL-1), as well as IL-6,
IL-11 and TGF-β, were upregulated in several cancer types and contributed to the lethal phenotype.
What determines whether patients start to produce these cytokines and embark on their fatal course?
“These analyses suggest that multiple cytokines/combinations of cytokines cause morbidity and mortality for cancer patients and offer multiple avenues for therapeutic development that need to be addressed,” wrote Pienta, adding that no single cytokine or subset was upregulated in all advanced cancers.
Other unanswered questions include whether the harmful cytokines arise from the tumour itself, or the microenvironment surrounding the tumour, or both, and what determines whether patients start to produce these cytokines and embark on their fatal course.
In the intervening 12 years since Pienta’s review was published, it is noteworthy that there have been few studies exploring the complexity of the final common pathway, and that Pienta himself has moved on to better funded avenues of research, such as studying the tumour microenvironment.
Cachexia
One of the few areas that has received research attention is cachexia, a wasting condition combining loss of skeletal muscle and adipose tissue in patients with late-stage cancer. Here a complex cascade of cytokines act on multiple targets leading to biological responses that culminate in progressive weight loss, anorexia, anaemia, depletion of lipids, and severe loss of skeletal muscle. However, the majority of cachexia trials targeting cytokines have not achieved positive outcomes. “The reason these antibody trials failed is that no one undertook the precision medicine approach of measuring which cytokines were raised in specific patients,” says Pienta, who believes there is widespread variability in cytokine production between individual patients.
Taking a multi-modal intervention approach that does not target specific cytokines, but instead addresses the multifactorial pathophysiology to reduce inflammation, says Kaasa, may prove more successful. The MENAC study, which Kaasa is undertaking with Marie Fallon from the Edinburgh Palliative and Supportive Care Group, in Scotland, is combining omega (n-3) polyunsaturated fatty acid supplements and nonsteroidal anti-inflammatory drugs (NSAIDs) to target inflammation, with a light exercise programme to strengthen muscles (clinicaltrials.gov identifier NCT2330926).
Taboos and ethics
The low priority placed on end-of-life research has its origins in society’s cultural discomfort with death. Medical researchers prefer to focus on prevention and cure, with some oncologists viewing death of their patients as professional failure. Conducting studies on the dying has been controversial, with a traditional view that patients should not be exposed to research at such a sensitive stage in their lives. “From the point of view of clinical studies, end of life is a very challenging area. Patients are often frail, they have multiple physical problems and can experience rapid and unpredictable deterioration,” says Marie Fallon, from the Edinburgh Palliative and Supportive Care Group, Scotland.
But people who are dying often welcome the opportunity to share their stories, reflect on their experiences, and contribute to knowledge generation, she says. An Australian integrative review of 10 studies concluded that patients with little time left often expressed the view that “it was important that they used that time to do something of enduring value,” and that they wanted to help others who may be in a similar position in future (Palliat Med 2018, 32:851‒60).
The phase III study, which in April 2015 started recruiting patients with incurable lung and pancreatic cancer who were at high risk of developing cachexia, is unusual for a palliative care study, in that it involves a number of centres in Norway, Sweden, UK, Canada and Germany. Having multiple centres, each providing access to local funding opportunities such as university grants, has proved key to their success in financing a trial of this size, says Kaasa.
In addition to exploring efficacy of this approach in cachexia, Kaasa hopes their collaborations with basic scientists reviewing blood samples taken from patients enrolled in MENAC will shed more light on the terminal biochemical pathways.
Predictive biomarkers
Seamus Coyle, who is unusual in being a palliative care consultant with a PhD in cell and molecular biology, is taking urine samples from patients in their last few weeks of life to identify metabolites that can be used as biomarkers to predict how long patients have left. While the study could provide valuable information for patients and their families needing to make plans, Coyle believes it could also provide additional insights into the fundamental biochemical pathways involved in the end of life.
“Knowing the metabolites that change towards the end of life is helping us to identify biochemical pathways that change during the dying process,” says Coyle, who received some initial seed funding from the Wellcome Trust health research charity, but then experienced a period of three years of working in his own time before receiving some funding from his own St Helens and Knowsley Hospitals NHS Trust in Liverpool.
At the European Palliative Care Research Centre, recently relocated from Trondheim University Hospital to the University of Oslo, Kaasa is developing plans for additional multicentre palliative care trials, including testing the efficacy of a ghrelin receptor agonist in cachexia and opioids in neuropathic pain, as well as intervention studies in brain metastasis. “Multicentre studies are essential to recruit the large samples of patients that are needed for external validity of studies,” he says.
Making the biology of cancer death a priority
One of the big challenges, according to Kaasa, is the lack of scientists equipped with the skills for basic biological research in the field, which he says is part of a self-perpetuating vicious cycle. “The lack of trained investigators makes it challenging to find suitable referees to review grants and papers, and we’ve problems identifying enough qualified MDs with end-of-life research experience to hold chairs in palliative care,” he says.
A survey by José Miguel Carrasco, from the University of Navarra, in Pamplona, Spain, identified only 50 full professors of palliative care across the 43 (out of 53) WHO European Region countries who responded (J Pain Symptom Manage 2015, 50:516–23). “If medical schools don’t have chairs of palliative care, there’s no one to champion the cause for the undergraduate medical school curricula, yet further reducing the likelihood of having people sufficiently experienced to do research,” says Kaasa.
The European survey revealed that 14 countries (33% of those who responded) did not include palliative care in their medical school curricula.
This vicious cycle is exacerbated by the lack of profile of the research that is actually happening in this field. Irene Higginson, from the Cicely Saunders Institute, points out that, “When investigators try to secure grants, they often hide the term ‘palliative care’, to make the study more appealing to funders.” This can make it hard to identify such studies using PubMed and Google search, which can be confusing enough because of the many and overlapping terminologies that are used, such as palliative care, end-of-life care, supportive care, personalised care, patient-centred care, or psycho-oncology.
“Research on the basic science of death needs to be embedded in a continuum of oncology research”
Kaasa, who chairs the ESMO group for Integrative Oncology and Palliative Care, has ambitions to establish a biannual ESMO conference dedicated to palliative care research in oncology, with a strong emphasis on biological science. “People do present palliative care biological research at ASCO and ESMO, but it just disappears in the big programme,” says Kaasa. The European Association of Palliative Care holds a biannual meeting, he adds, but that conference caters for all areas of medicine, and not just oncology.
“To really develop understanding of the biology of cancer death we need to establish a new forum that will attract clinicians and basic scientists from all over the world. It’s by coming together that we can scope the range of research that’s already taking place, and achieve a critical mass of investigators to establish research priorities to advance the field, nurture the next generation of scientists and start to give this vital area of medicine the priority it deserves.”
Marie Fallon, from The Edinburgh Palliative and Supportive Care Group, argues that research on the basic science of death should not be hived off into some specialist niche, but needs to be embedded in a continuum of oncology research. “You can’t just look at patients in the last few weeks of life when they’ve exhausted all available treatments. You need to understand how the biology evolves throughout the disease trajectory,” she says, adding that if investigators only consider patients who have failed chemotherapy, they are looking at biased samples. “To really understand what is going on, we need to review the whole group and understand the relevance of different patient phenotypes.”
Kaasa agrees: “We need to understand the host’s reaction to the cancer both at the start of the disease trajectory and at the end of life. It’s only with such knowledge that you can start to understand why cancers kill some people and not others.”
A new platform for end-of-life research
France has taken up the challenge of end-of-life research with the establishment, in October 2018, of a national platform, part funded by the French Ministry of Research and French Ministry of Health, to provide an infrastructure to boost palliative care studies.
One of its first steps was to identify relevant investigators, by means of a survey. “As we had little idea who was out there, we used a chain letter approach, where we asked respondents to pass the questionnaire on to anyone else they knew who was working in the field,” explains Elodie Cretin, the director of the Platform, who is a research coordinator for the French Institute of Health and Medical Research (INSERM) at the University of Besançon. “We’re currently analysing around 300 responses and hope to use this information to identify research priorities and to create an online directory that will enable investigators to connect with each other.”
Additional plans for the platform include lobbying charities and government agencies, such as the French National Society for Cancer, for funding, and providing young investigators with training on research methods, how to write papers, and the special ethical considerations that need to be taken into account.








Leave a Reply