P Hadji, R E. Coleman, C Wilson et al. (2016) Adjuvant bisphosphonates in early breast cancer: consensus guidance for clinical practice from a European Panel. Ann Oncol 2016, 27:379–90
Bisphosphonates should be considered as part of adjuvant breast cancer treatment in postmenopausal women, or those receiving ovarian suppression therapy, and the potential benefits and risks should be discussed with relevant patients. This consensus statement, published earlier this year by a panel of 26 experts, gives new evidence-based guidance on the use of a class of drugs that could prevent one in six deaths among postmenopausal women with early stage breast cancer, and are effective against breast cancer related bone loss — but are not approved for either indication. Janet Fricker spoke to Robert Coleman, lead author of the consensus paper and meta-analysis, to ask him how the consensus statement came about and what obstacles women across Europe face in getting access to this potentially life-saving treatment.
Janet Fricker: Research indicating a possible role for bisphosphonates in treating breast cancer has been around for more than a decade. Why did you feel now was the time for a consensus statement?
Robert Coleman: The idea that adjuvant bisphosphonate therapy might prevent the spread of breast cancer goes back 15–20 years and encompasses both preclinical animal studies and clinical trials.
In the 1990s, two trials reported a reduction in bone recurrence and improved overall survival for the bisphosphonate clodronate (Ann Oncol 2008, 19: 2007–11; Breast Cancer Res 2006, 8:R13), while a third study suggested adverse effects for clodronate, including increases in extra-osseous metastases (Acta Oncol 2004; 43:650–56).
Robert Coleman is Professor of Medical Oncology at the University of Sheffield, UK
Initially, the reasons for such conflicting outcomes were unclear. When we came to design the AZURE trial [Coleman was first author], looking at the intravenous bisphosphonate zoledronic acid, we planned an exploratory subset analysis according to the women’s menopausal status at the time they started treatment (Lancet Oncol 2014; 15: 997–1006). Since it is well known that bone metabolism changes as women age, it seemed only sensible to explore outcomes according to menopausal status.
Our results showed that while there was no overall benefit from adding zoledronic acid to standard adjuvant treatments in early breast cancer, treatment reduced the development of bone metastases in the subgroup with established menopause, delivering improved invasive-disease-free survival for women who were over five years since menopause at trial entry (HR 0.77, 95%CI 0.63–0.96).
Similarly, the NSABP-3 study investigators, who looked at the effects of the bisphosphonate clodronate used as an adjuvant treatment in operable breast cancer, included a subgroup analysis where outcomes were compared for women aged 50 years or more at study entry with those who were younger. Again, recurrence-free survival benefits were found for the older age groups (Lancet Oncol 2012, 13:734–42).
Together, such studies led to the theory that bisphosphonates might exert their anti-cancer benefits solely in postmenopausal women. Supporting this hypothesis, preclinical data have demonstrated improved efficacy of bisphosphonates in preventing bone metastases against the background of low levels of female and male hormones.
One study, which compared the effects of zoledronic acid (100 µg/kg weekly) on growth of disseminated MDA-231 breast cancer cells in bone between ovariectomised mice (modelling menopause) and sham operated mice (modelling premenopause), found the number of bone detectable tumours only decreased in ovariectomised mice (Clin Cancer Res 2014, 20:2922–32).
To clarify the issue of whether menopausal status affects bisphosphonate efficacy and to investigate available evidence in a more ‘robust and precise’ fashion, The Early Breast Cancer Trialists’ Collaborative Group (EBCTCG), co-ordinated by the University of Oxford, undertook a meta-analysis of all unconfounded randomised trials comparing breast cancer outcomes in women who were allocated adjuvant bisphosphonates versus those who were not. The meta-analysis involved 18,766 women from 26 separate bisphosphonate trials, and was published in the Lancet in 2015 (vol 386, pp 1353–61).
The results showed that, among the 11,767 postmenopausal women, bisphosphonates produced highly significant reductions in recurrence (RR 0.86), distant recurrence (RR 0.82), bone recurrence (RR 0.72) and breast cancer mortality (RR 0.82).
Among premenopausal women, treatment had no apparent effect on any of these outcomes. Risk reductions for relapse and mortality in postmenopausal women treated with bisphosphonates, furthermore, were found to be similar irrespective of ER status, grade of the primary tumour, axillary lymph node involvement, and whether or not chemotherapy was used.
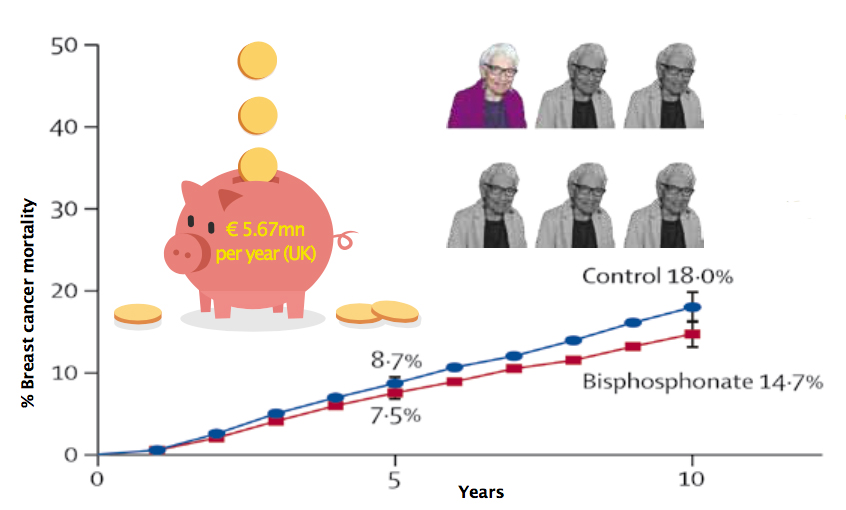
Overall, the results show that, for postmenopausal women, this low-cost treatment, which for zoledronic acid has been calculated to cost just a few hundred euros for the entire course of treatment, would reduce the risk of dying from breast cancer by 18% – more than one woman in six – in the first 10 years after diagnosis.
After the Lancet meta-analysis paper, we were left with a clear result for a group of drugs that do not have regulatory approval for the indication of preventing metastasis. We therefore felt that it would be valuable to produce a strong consensus statement giving clinicians confidence to prescribe these drugs for their patients. We also felt that the statement could be used to provide evidence to convince funding committees about the benefits of bisphosphonates in post menopausal women with early breast cancer.
While ESMO has published the Clinical Practice Guideline ‘Bone Health in Cancer Patients’ (Ann Oncol 2014, 25 Suppl 3:124–137) [Coleman was first author], this document addresses all cancers and only offers a few sentences on the use of bisphosphonates in breast cancer to prevent metastasis. We felt that it was important to develop a longer document providing more space to this important topic. We also felt that it was particularly important to publish our conclusions in an oncology journal, rather than a general medical journal, as this would help reach the wider oncology community.
JF: What is the scientific rationale underlying this clear benefit in postmenopausal women with early breast cancer?
RC: Even now we don’t fully understand the mechanisms behind why bisphosphonates prevent bone metastases only in postmenopausal women. Our front running theory is that the postmenopausal state results in increased bone turnover, which could potentially lead to excess production of growth factors from bone, which in turn may favour survival of disseminated tumour cells or micrometastases within the bone marrow microenvironment. Through their inhibitory action on osteoclasts and slowing down of bone turnover, bisphosphonates could in theory reduce expression of these factors, and thereby prevent the establishment of micrometastatic disease.
JF: How did you go about producing the consensus document?
RC: For the consensus we got together an ad hoc group of 26 key opinion leaders, inviting representatives across the fields of both breast cancer and bone health to participate. To provide an unbiased overview, we took care to involve a number of experts who had not been involved in any of the earlier bisphosphonate breast cancer trials.
Using the nominal group methodology for consensus, a systematic review of the literature was undertaken using Pubmed and Medline databases from 1970 to 2014. Our start day took into account the fact that bisphosphonates were only recognised to have any medical uses in 1968. Conference proceedings from the San Antonio Breast Cancer Symposium, European Society for Medical Oncology and the American Society of Clinical Oncology from 2000 to 2014 were also included.
Our reasoning here was that many small studies presented at meetings do not reach the peer reviewed literature. In addition, the panel had access to the EBCTCG meta-analysis findings before publication. The literature was supported by a face-to-face meeting in October 2014. After presentations and structured discussions, participants voted on a series of questions that had been specially developed to consolidate expert opinion and address all the practical questions it was felt clinicians would want answered.
Answers to questions took the format of ‘agreement’ or ‘disagreement’, with responses graded ‘strong’, ‘slight’ or ‘neutral’. We felt that it was important to develop a five-point scale, since thinking in clinical medicine is rarely black and white, and there is a need to represent the shades of grey, and highlight areas where there are still questions to be answered.
For the consensus we included additional information about preventing treatment-related bone loss, which was non-contentious, since we felt for ease of access it was important to gather all the information on breast cancer bone health together in a ‘one stop shop’.
The meeting received funding from the German BANSS Charitable Foundation, who covered travel expenses for the panel and support for a medical writer.
Adding bisphosphonates saves an additional 1 life in 6
and works out cheaper in the longer run
JF: What recommendations did the panel make?
RC: The consensus panel recommended that bis-phosphonates (either intravenous zoledronic acid or oral clodronate) should be considered as part of adjuvant breast cancer treatment in postmenopausal women or those receiving ovarian suppression therapy; with some experts (58%) suggesting its use should be further restricted to those considered at intermediate or high risk of recurrence rather than across all risk groups. This view takes into account the risk–benefit ratio, where the risk of recurrence in some women is considered so low that it is not worth the possible side effects, such as osteonecrosis of the jaw.
JF: What is the situation regarding access to bisphosphonates for use in adjuvant treatment of early breast cancer?
RC: In Europe access to bisphosphonates to prevent metastasis in early breast cancer varies from country to country, resulting in major inequities in care. I understand that Germany and Austria introduced treatment last year, but that the treatment is not yet available in countries like Italy and France.
In the US, drugs that are not licensed are not reimbursed by insurance companies, so patients essentially have to fund these treatments out of their own pockets.
In the UK there is a postcode lottery, where clinical commissioning groups in some areas have agreed to fund bisphosphonates for this purpose, but others have not. A survey by the UK Breast Cancer Group of 125 breast cancer oncologists found that three out of four respondents had not been able to implement bisphosphonates for their early breast cancer patients.
One of the key issues determining access is that bisphosphonates used in breast cancer have been ‘repurposed’ and do not have licenses for the indication of preventing breast cancer recurrence. Achieving regulatory approval for a new indication for repurposed drugs would require submission of all the relevant clinical trial data in the appropriate format to the regulatory authorities and, because pharmaceutical companies do not anticipate a return on drugs that are off-patent, or soon to be off-patent, there is reluctance to fund this process.
While doctors can already prescribe ‘off-label’, when they consider it in the patient’s best interests, in practice they may be deterred by the potential personal liability they may face in doing so. Furthermore, such ‘off-label’ treatments do not make it into national formularies, with the result that they are not considered by health technology assessment bodies (such as the UK’s National Institute for Health and Care Excellence) who assess the clinical and cost effectiveness of treatment. This is significant, since a positive decision is often considered a prerequisite before commissioning bodies will agree to fund drugs.
In the UK the ‘Off-patent drugs bill’, which failed to get through parliament in November 2015 after being filibustered (the practice of delaying legislation by making long speeches), would have put into law a duty on the UK government to take steps to secure marketing authorisation for repurposed drugs when pharmaceutical companies will not, followed by a requirement for NICE to conduct technology appraisals. The issue remains under discussion between interested ministers and advocates across a range of disease areas but does not appear to be an urgent government priority.
We want the message to get through to commissioning authorities that, irrespective of the humanitarian aspects of making these treatments widely available, use of bisphosphonates to prevent recurrent breast cancer makes good economic sense.
In Sheffield, we have recently developed a business case showing that giving bisphosphonates to patients with early breast cancer saves money in two ways. First you don’t have to perform expensive bone density scans, and second, if women do not get recurrent breast cancer this saves the costs of treating advanced cancers.
Assuming the whole cohort of 35,700 postmenopausal women with invasive breast cancer are treated in the UK, we calculated that this would result in treatment costs of £16,917,783, which would be offset by savings of £6,835,122 from no longer needing to perform DEXA scans, and further savings from needing less treatment for secondary breast cancer of £15,173,500, leading to net savings of £5.09 million [€5.67 mn] per year (see http://breastcancernow.org/information-for-clinicians-about-prescribing-bisphosphonates). But, from the point of view of a commissioner trying to balance their books, that financial benefit will not be accrued for quite a few years.
The case for bisphosphonates in postmenopausal early breast cancer
A meta-analysis involving 18,766 postmenopausal women with early breast cancer from 26 separate unconfounded randomised controlled trials (Lancet 2015, 386:1353–61) showed treatment with bisphosphonates lowered the mortality rate over 10 years from 18% to 14.7%, which amounts to saving an additional one in six lives – around 10,000 lives a year in Europe. A financial analysis conducted by the South Yorkshire Cancer Strategy Group showed that the savings made from reducing the number of women who need to be treated for advanced breast cancer, and from not having to perform DEXA scans to monitor bone density, outweigh the costs of using bisphosphonates as a routine part of adjuvant treatment of postmenopausal women with early breast cancer, saving the UK health service around €5.67 mn a year
JF: What has happened since the consensus statement and what studies are ongoing or being planned?
RC: Since the consensus there have been additional trials including the SWOG0307 trial, which addressed whether different bisphosphonates have similar efficacy. The study, presented as an abstract at ASCO 2015, randomised 6,097 postmenopausal patients with stage I–III breast cancer to receive oral clodronate (1,600 mg/day) or oral ibandronate (50 mg/day), each for three years, or intravenous zoledronic acid (4 mg/month for 6 months, then every 3 months for 2.5 years). Results showed that disease free survival and overall survival did not differ between the arms, but that there were slightly more cases of grade 3/4 adverse events with ibandronate (10.5%) than clodronate (8.3%) and zoledronic acid (8.8%).
The SUCCESS trial, comparing five versus two years of zoledronic acid in 3,800 patients, is due to report soon and should give important insight into duration of treatment. My personal bias is that bisphosphonates exert their beneficial effects early on in the disease process, and there won’t be any additional advantages in giving drugs much beyond two to three years.
Interestingly, the Z0-FAST study, looking at cancer treatment induced bone loss, reported fewer recurrences in women receiving immediate zoledronic acid than in the control group, where bisphosphonate was only introduced months or years later (Nat Rev Rheumatol 2013, 9:365–74). To explain the upfront effect I use the analogy of grass seed where to be effective in preventing grass from germinating it is necessary to stop it taking root in the first place. Once established, however, perhaps like disseminated cancer cells, grass becomes very resilient to damage.
We will present the 10-year results of the AZURE trial in San Antonio this coming December which will give us more information on the long term benefits of treatment and may provide insights into whether women who became menopausal as a consequence of chemotherapy go on to benefit from bisphosphonate treatment.
Other trials of interest include the UK IBIS III trial (www.ibis-trials.org), run by Jack Cuzick, which will look to compare the effectiveness of metformin, zoledronic acid and aromatase inhibitors in preventing breast cancer returning in women who had their breast cancer diagnosis more than five years ago but remain at risk for recurrence of disease. We also want to continue following up patients from existing trials to see whether use of bisphosphonates has an effect beyond 10 years and influences subsequent metastases beyond bone. Ultimately we hope to build up a map showing how cancer progression is influenced long term by bisphosphonates.
The D-CARE study is exploring whether denosumab, a synthetic humanised antibody to a molecule called RANK ligand, regulating osteoclast function, can also provide benefits in early breast cancer. The big hope that Amgen have for denosumab, which is still well within patent, is that they will be the only company to get regulatory approval for the indication of preventing breast cancer recurrence.
To my mind there’s a real danger that we could end up spending a factor of 50 to 100 times more on a newer agent like denosumab simply because we don’t have a piece of paper that gives regulatory approval to use generic bisphosphonates, despite their extremely strong evidence base.
As the results of these trials are published, it will be important to update our consensus document with the new information. While we do not yet have any formal plans, we would very much like any future consensus to come under the umbrella of a major organisation, like ESMO, and would also like to invite representatives from North America to take part, to extend our consensus across the world. Ultimately we believe such endorsements would give us additional credibility in convincing drug funders of the urgent need to get these extraordinarily cheap life-saving drugs to patients.