If your ambition is to excel at the oncology career you have chosen, you have to find your own pathway to success. Anna Wagstaff talked to three early-career oncologists who are trying to do just that, and asked them what worked, what didn’t, and what tips they have for others who are determined to be the best they can be.
Assia Konsoulova, a medical oncologist at the Burgas cancer centre in Bulgaria, does not specialise primarily in gastrointestinal cancers. So when some patients with locally advanced gastric cancers were assigned to her care, she tried to refer them to specialists who could offer them neoadjuvant therapy, which the evidence indicates could improve their chances.
But neoadjuvant chemotherapy was hardly ever used in Bulgaria for gastric cancers, and no one wanted to do it, because of the greater complexity, the response assessment, and the potential added risk.
So Konsoulova decided she would take on the responsibility, and she managed their care herself. “And I proved that, just as it says in the literature, it works.”
Younger colleagues then followed her lead, she says. “They were motivated, so now I transfer my gastric cancer patients to them, and we work together, and as a result they are now building up their specialist experience.”
What made Konsoulova go the extra mile for these patients when others wouldn’t?
Her specialty is breast cancer and neuroendocrine tumours, so it was clearly not superior knowledge. She cares deeply for her patients – but the same can be said for very many medical oncologists in Bulgaria.
What made the difference, in her view, was the experience and confidence in her own capability as a doctor that she had gained through a continuous search to learn and improve, which had included – crucially – spending time gaining hands-on experience in specialist centres abroad.
You’ve got to make it happen
Konsoulova realised early in her career that if she wanted to be a great cancer doctor she would need to go out and look for the experience and knowledge she needed. “When you start, for every young doctor it is not easy. You get lots of duties, lots of paperwork, night shifts, and then at some point you realise that your dedicated oncological education is not really happening.”
She applied for an EU scholarship to the Jules Bordet Institute in Brussels, and says the experience totally changed her idea about her chosen career. “I understood what oncology is really about – not just prescribing drugs and measuring response. It is care for patients, it is management and organisation, it’s a way of thinking.”
It was at the Bordet Institute that Konsoulova got her first experience in the art of medical decision making. “I had a personal supervisor, who would ask me: “What would you do in that patient?’ ‘What would you expect in that patient?’ I had the chance to look at patients as their treating oncologist, to discuss with colleagues and then decide on the best options, and argue the case for my decision. And I was taught to always follow patients through to the present, to learn about whether previous management decisions had been right or could have been improved, so that you always learn from experience.”
Konsoulova returned to her post in Bulgaria, where she did her best to implement the new approach she had learnt. Over the next 10 years, she systematically built up her competences by travelling to attend practice-oriented courses in clinical and medical oncology, as well as more dedicated courses about managing neuroendocrine tumours and breast cancer. Most recently she spent six months at the Champalimaud cancer centre in Lisbon – an international leader in breast cancer – where she also got the chance to further develop competence and skills in clinical research.
“The benefit of that education gets bigger the more you already know. You need a solid background”
“I was writing protocols, learning what was published during the previous month, and immediately discussing its relevance to clinical practice. There were, for instance, Journal Club sessions where, on a rotating principle, we would present what was new and relevant in the field, to really stay updated every single week. All relevant information was considered at the multidisciplinary team discussions and introduced into the patient management.”
While the topic was breast cancer, the approach, the expertise and the confidence related to oncology practice in general. So when Konsoulova returned home again, she felt able to respond to the needs of her patients with gastric cancers, while colleagues specialising in those cancers did not.
“Training is not something that starts and ends. It continues for life,” says Konsoulova. “Every time I go abroad for a course or a specialisation, I see that I’m getting better, but the benefit you get of that education is getting bigger the more you already know. You need to have a solid background. The improvement is much more significant the more you are advanced with your knowledge.”
Get a good foundation
In neighbouring Turkey, Hakan Buyukhatipoglu, now working as a medical oncologist in Adana, took a similarly proactive approach to his own education and training. His ambition is to work at the frontiers of clinical knowledge, designing and conducting trials in his specialist field of breast cancer.
To that end he has spent years looking for courses and fellowships and other training opportunities, learning from the people around him, as well as reading, reading and more reading.
Like Konsoulova, he stresses the importance of starting by building a solid background in oncology. For him, this comes down to three essentials: First comes molecular oncology, which he says is not much included in medical oncology training, yet is key to accurate diagnostics and to understanding the rationale behind different treatment approaches. Buyukhatipoglu did a partially grant-funded cancer biology course offered by Harvard, but says there are other good options available in Europe.
Second comes radiology – also not included in medical oncology training. Having some knowledge of how to read and interpret images is important, he says, particularly when you are comparing before and after treatment. “There are a lot of courses available online and at medical schools,” says Buyukhatipoglu, but he chooses to study this alone – and learns by discussing his cases with radiology colleagues.
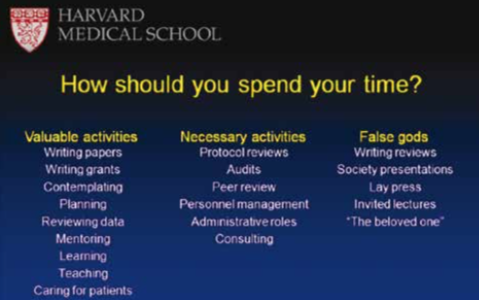
Of the hundreds of powerpoint slides Hakan Buyukhatipoglu has encountered during his educational journey, this is the one he values the most
The third essential, in his view, is a grounding in clinical trials biostatistics, because oncology guidelines are based on clinical trials and studies. “If you want to draw some conclusions you have to have some knowledge about biostatistics. Why is this study important? How was it done? Is the design correct? How was the patient selection done? Was it randomised? How was it interpreted? This is really important.”
Buyukhatipoglu loves learning and, beyond his own specialism, has spent time learning about pulmonology, radiology, radiation oncology and psychology, and incorporating that knowledge into his practice. But with so much to learn it becomes very important to know how to use your time wisely. The single presentation slide he feels has helped him most is about how young doctors should prioritise their activities.
You’ve got to want it
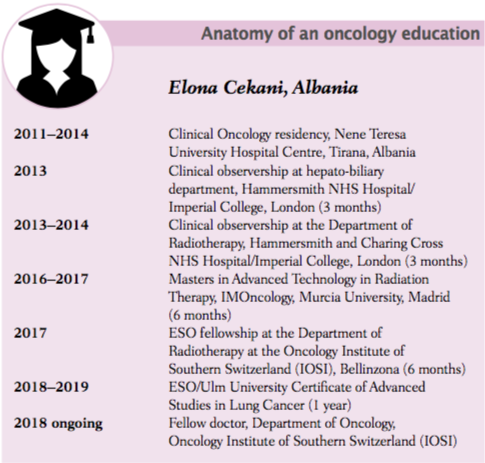
“I think the life of a doctor, especially from a poorer country, is running around with your handbag, and a small luggage on your shoulder, and then getting educated. You cannot be properly educated until you reach your 40s, and everyone should know it is like this.”
So says Elona Cekani, who did her initial training in Tirana, Albania, but has spent much of the past six years travelling around Europe to build the knowledge and experience she needs to be confident of giving her patients the best possible treatment and care.
As a ‘clinical oncologist’, Cekani needs to master both medical and radiation oncology. And in a country that is only just beginning to organise cancer care along specialist lines, she needs a good grounding across the major cancers, while also pursuing her specialist interest in lung cancer.
“It is very simple if you have a structure, an institute, a university, that tells you: this is your curriculum, you have to do this, you have to have this exam and then you go and perform everything that you have been told. It is very difficult to go around Europe and look for what you need, and to see what you are missing and look around to see how you can fill the gaps. Especially when you don’t have financial support and you are always hunting grants and fellowships.”
Cekani has invested an immense amount of her time filling out applications, and studying the literature to find gaps where she could propose a research project that might win her a research grant or fellowship in a leading centre.
Good experiences include six months in Madrid doing a Masters degree in advanced technology and radiation therapy. “I was taking part in the decisions, discussing cases and being able to see these patients and visit them with my supervisor, as part of a team.” She learnt “all the basics” involved in radiotherapy, and also trained in stereotactic (multi-directional) radiation therapy – expertise that she says she can use on returning home, as “you can now do it even with a linac”.
The experience also taught her that she needed a better grounding in medical oncology, which led to another good, hands-on experience working as a fellow at IOSI, the Oncology Institute of Southern Switzerland, where she is completing a series of rotations in the main cancers and in palliative therapy, which she sees as an essential part of her training.
However, successful applications didn’t always turn out as she’d hoped: Cekani had some very mixed experiences with visits to institutes based on watching rather than participating. “I can say that observership periods are generally not useful. When you go to countries that are much more developed than yours, you expect a lot, and you sacrifice a lot to be in these training programmes. Unfortunately I have seen sometimes that people don’t know what to do with us. I couldn’t orient myself very well and there was a lot of empty time, and that is not very useful for a young doctor. When you get the chance for hands-on participation, this is very different.”
The attitude of your supervisor is important, she adds, and she advises potential applicants to get in touch with them before travelling. “Understanding their background, having an interview with them, seeing how eager and passionate they are, can help you a lot. Then you get the first impression of whether you are going to go around corridors in your empty time or whether you are sharing your passion with your supervisor.”
Don’t rely on a mentor
While Cekani feels let down by some of the people who were tasked with supervising her, she has often found great support and mentorship from people with no formal responsibility for her training and from colleagues and teams she was working with. “Getting a proper network around you helps you a lot. Often I have seen people who inspire me to innovate, create, strive for perfection, practise a lot. …Working in different structures in different hospitals, you get a sense of what is working and what is not. It’s about never losing your critical sense, and being able to get the best from everyone.”
Cekani makes special mention of the role of online communities as rich sources of discussion and knowledge sharing. This is something she first experienced while in Spain, where she joined a Whats-App group that included more than 300 doctors.
She had some very mixed experiences with visits to institutes based on watching rather than participating
“Everyone was discussing cases with colleagues all around Europe and the world. It was very helpful, because every time somebody gave you an opinion, they sent the articles they were basing that opinion on. I’ve learnt a lot from them and I’m still trying to practise this kind of learning.”
While social media is not an alternative to multidisciplinary team work, she says, “it is something useful that everyone can do in their own country, even in developing countries.”
Make your own choices
As Scientific Director of the European School of Oncology, Fedro Peccatori’s job is to help young oncologists become the best cancer doctors they can be, principally through the courses, fellowships and online teaching offered by the School. He argues that having a great mentor can help guide your understanding of what is important and what isn’t. But he cautions that they are a rare commodity, and there are dangers in depending on other people – no matter how eminent or well-intentioned – to tell you how to develop your career.
“You have to understand what is important yourself. So you have to be proactive, and interact with your mentor and sometimes explain to them what is important to you. You shouldn’t just be passive and say, ‘I’ll do what the professor told me because he is a very important big professor.’ Everybody at times would like to have someone who acts as a navigator for them. But it’s up to you to decide what you need, be that a particular specialism or veering more towards research or whatever excites you.”
Peccatori speaks from experience. He started his career fascinated by the scientific challenge of cancer, in the days when advances in molecular biology were beginning to reveal the intricacies of the disease. But along the way, his focus on excelling in pathology altered, not because his love of scientific exploration waned, but because he wanted to work with patients. “So I changed my mind and I said, maybe I’ll do something more clinical.”
Decades later, Peccatori is very pleased he made the decision he did, and shifted his career path from a predominantly scientific focus towards developing knowledge and experience in providing cancer care for women who want to preserve their fertility – a passion he continues to pursue part time at the European Institute of Oncology in Milan.
“Every young oncologist must feel their way towards their chosen path, and pursue it as best they can”
The decision to opt for a career as a hands-on doctor in his chosen specialist area was the right one for him, he stresses, and it is up to every young oncologist to feel their way towards their own chosen path, and pursue it as best they can – “It’s very personal.”
Learn to care
Patients need a doctor with the knowledge to do the best for them. But if that doctor doesn’t take the time and empathy to understand that patient, the pressures they face, their values and priorities, that knowledge won’t translate into the best care, says Peccatori. That is why the motto of the European School of Oncology is ‘Learning to care’, “not ‘learning the latest molecular mechanism’, not ‘learning to treat cancer’ – important though that is”.
Patients want oncologists to be present for the long term, he says, whether or not the cancer is curable. “The impact of cancer and treatment can last a long time, and doctors need to support their patients and also learn about long-term effects that would otherwise go undocumented.
“We see a lot of excellent oncologists who are not truly great oncologists because they forget how important it is to establish a true relationship with their patients.”
This is asking a lot, admits Peccatori, because oncologists work under pressure, “We are human beings, we are distracted, sometimes we are stressed, and tired, and burdened with a high administrative workload.”
A bigger challenge, perhaps is the nature of the doctor–patient relationship in oncology. “Cancer puts a very strong burden on the patient – probably more than any other disease – because of the perception of how cancer impacts on your daily life, even if you are cured… You are standing in a position where you have the knowledge, you are healthy, you sometimes have the power to decide whether this drug can be given or not, whether a patient can go on that protocol or not.
“It is difficult to handle well if you are not very keen to understand and take responsibility for this oblique relationship.”
“Great clinical judgement can only come with practice. It’s why ESO encourages young oncologists to travel to get hands-on experience”
It’s about wanting to be a great human being, and not just a great doctor, says Peccatori.
But can that be taught? “Everything can be taught, and everything can be learnt,” he says. “We teach by example.”
He mentions as an example the ESO–ESMO Masterclass in Clinical Oncology, which lasts five days and starts with a full day on communication skills, where oncologists and cancer nurses learn side by side – “That is so important”. It allocates time to discussing real patient cases, submitted in advance by participants, to demonstrate the process of working out the best options and how to convey choices to the patient.
Great clinical judgement, says Peccatori, can only come with practice. It’s one reason why the School is so keen to encourage young oncologists to travel to centres to get hands-on experience.
As one of the young oncologists who took advantage of such opportunities, Assia Konsoulova describes how she learnt the difference between treating patients and caring for them.
In Bulgaria, she says, she felt that the task of the doctor was to see the patient for a certain ‘problem’ and solve that particular problem.
By contrast, her experience while at the Jules Bordet Institute and the Champalimaud, was that, “the patient is seen as someone with a chronic disease who you will see and care for along the years. So when considering a certain treatment, you discuss the patient – their comorbidity and potential prognosis – you discuss potential options and evolutions, and the patient’s preferences and their expectations.”
She decided staying at her prestigious hospital would not give her the opportunity to be the great doctor she wanted to be
Multidisciplinary meetings were “exceptionally different” to the discussions she was used to at her home institution, which would rarely last more than a few minutes.
“We as caregivers become a part of their life as we treat their disease. We don’t simply treat the cancer, but the patient with cancer. This is a really different way of thinking.”
No boundaries no barriers
Roger Wilson has been living with cancer almost since Konsoulova started at medical school. He learnt about the damage done by incompetent management when he was first operated on without any of the diagnostic tests required to establish that the lump in his leg was cancerous.
He has played a leading role in initiatives to give patients and advocates a greater voice in decisions affecting care, including at the level of research and the way care is accessed and delivered. He is one of two patient advocates who are on the faculty of the week-long workshop on Methods in Clinical Cancer Research run by EORTC, ESMO, ECCO and the AACR, where he helps participants think about how to incorporate patient perspectives into their trial design.
What does Wilson want from his oncologist? “I expect them to have all the background that they need to address the issues that I am presenting with. I want them to be a doctor. I want them to be caring. I want them to have empathy. I want them to have an understanding that they are not treating a disease they are treating a patient. I want them to be able to work with the other staff – usually a nurse in attendance – with an understanding on both sides that they are working towards a common end.”
Wilson knows full well how hard it is to do all of that, particularly in the current era. “The feeling I have is that chemotherapy and the traditional cytotoxic route was still very disease oriented not patient centred. And as we’ve moved into precision medicine, the science is so mind boggling we are actually moving into a biochemical-centred approach rather than even disease-centred, and the danger is that the patient is absolutely nowhere in this equation.”
He feels for young oncologists who are trying to master the science while keeping a grip on the essentials of being a great doctor. “They are taking on so much already, it is hard to see them coping with anything else.” The key lies in how their more senior colleagues behave, Wilson believes, because young doctors model themselves on what’s in front of them.
With decades of experience as a media producer, manager and company director before becoming a patient, advocate, and teacher, Wilson feels he has become good at picking out which junior oncologists will go on to lead teams and departments that deliver an outstanding service. “They have a sort of buzz about them. No boundaries, no barriers, taking responsibility for getting the best possible answer for the patient, rather than saying: this is my job.”
It’s an important point, not least for the many young oncologists who make an effort to learn new and better ways of working through visiting centres of excellence abroad, but then find it a struggle to put their knowledge and skills to good use when they return to their home institutions.
Konsoulova says that, on returning to her home institution, while many people acknowledged the value of the time she had spent gaining experience at international centres, others were quite hostile. “They say, ‘OK you were on vacation in Brussels or in Lisbon. Now you have to work more in order to compensate.’”
“Having an open mind is probably the single most important factor in becoming the best cancer doctor you can be”
She found it difficult to introduce a team approach to treatment and care, as there was resistance to anyone addressing problems outside their own immediate area of work. The attitude is “this is your job and this is not your job.” In the end, Konsoulova decided that staying at her prestigious university hospital, where her career was well outlined and heading upwards, would not give her the opportunity to be the great doctor she wanted to be.
She left, and moved to work in a large oncological centre where, she says, the management are ambitious to improve, “and are asking how best to do that.”
“I was invited as a specialist, to join a team of specialists and great oncologists. I have the opportunity to work and develop my career, to influence colleagues, the management, the policies, the decision-taking process on a long-term basis. So hopefully this will influence my career but also influence the decision-taking in the entire institution, which is finally what we are all fighting for.”
Cekani from Albania is also determined to implement new approaches in her home country. To keep her impressions fresh she keeps a diary – a tip she learnt from her father – and writes down first and second impressions, criticisms of herself, of others, and of the institute.
Otherwise, she says human nature is to adapt quickly and forget what drove you to start down a path. “Everything I’ve written down since I’ve started my training is how I can implement this and how I can improve this in Albania.”
She’s aware of the barriers, as team work, specialisation, patient-centred care have not been part of her country’s medical culture. Yet she remains very optimistic. “I’m always in touch with my friends and colleagues… I’m confident the new generation is changing… They are becoming more open minded,” she says.
For Cekani, having an open mind is probably the single most important factor in becoming the best cancer doctor you can be. Her advice to young oncologists is this: “Educate that beautiful mind of yours, and never stop questioning everything, thinking critically about everything, and discuss, discuss, discuss, because medicine is not an absolute science, it is a relative science. Everyone has to make their own decisions, but that must be based on the right training and education and keeping your mind open, because everything is changing so fast.”




 So Konsoulova decided she would take on the responsibility, and she managed their care herself. “And I proved that, just as it says in the literature, it works.”
So Konsoulova decided she would take on the responsibility, and she managed their care herself. “And I proved that, just as it says in the literature, it works.”