People with incurable cancer need doctors who offer them hope but also give them a clear idea of what is realistically possible. Doctors can find it hard to be both empathic and honest when the news is bad. Psycho-oncologist Lesley Fallowfield outlines the key issues that need to be addressed in consultations, and the pitfalls to avoid.
This grandround was first presented by Lesley Fallowfield, from Sussex Health Outcomes Research & Education in Cancer, Brighton, UK, as a live webcast for the European School of Oncology. Richard Simcock, from Sussex Cancer Centre, Brighton, UK, poses questions raised during the presentation. It was edited by Susan Mayor. The webcast of this and other e-sessions can be accessed at e-eso.net.
What are we doing when we communicate with our patients? William Osler (1849–1919) suggested, “The practice of medicine is an art, not a trade, not a business; a calling in which your heart will be exercised equally with your head.” One of the primary difficulties that clinicians face is achieving this balance.
Apart from the fact that patients deserve to receive good communication from healthcare professionals in any setting, good communication is necessary to ensure they can provide truly educated and informed consent to the management strategies they are offered.
Research has clearly demonstrated the value of effective communication. It is key to providing good clinical care and has beneficial effects on doctor/patient relationships. However, discussing a cancer prognosis and the complexity of modern diagnostics and treatments and therapeutic aims is not always easy.
There are many evidence-based courses to help doctors communicate in a clear, honest and empathic manner, but fewer on how to navigate the boundaries between personal and professional involvement with patients. One of the problems that has become increasingly apparent over the past few years is that encouraging doctors to get closer to the emotional needs of patients and their families puts them at psychological risk.
Key elements of good communication
Good communication in a clinical setting must include something on the therapeutic intent of treatment, such as palliation or controlling cancer when dealing with metastatic disease. Doctors are required to discuss all available options, including referral for supportive care. It is important to make sure patients understand everything that is involved in their treatment, such as treatment regimens and the visits required. In addition, it is essential to achieve the right balance in talking about the associated risks and harms of treatment compared to the likely benefits, as part of ensuring patients are able to give truly informed consent.
Encouraging doctors to get closer to the emotional needs of patients puts them at psychological risk
There is growing recognition of the importance of involving patients in decision making; however, this can be quite difficult in practice. The relationship between a patient and doctor is not symmetrical. Doctors have considerable power because of their knowledge, and they do not have to experience the consequences of treatment. A further ethical problem is that it can be difficult to genuinely share decision making with a patient if a doctor has a clear view, from a professional point of view, of what really would be in the patient’s best interests. It is also important to bear in mind that it can be difficult for a patient who is sick and anxious to convey their values, and aspects of their lifestyle, that impact on their treatment preferences.
Question: When you talk about psychological harm to doctors, can you explain the types of harm they might experience?
Answer: There has been a lot of work over the past decade looking at the levels of emotional burnout that many oncologists, in particular, experience. This is partly due to the fact that they are generally really empathic people. Doctors can sometimes be criticised for being cool, but some degree of detachment can protect them from being hurt. If you care about your patients you are inevitably going to expose yourself to trauma, particularly when sharing difficult news. However, at least we now talk about these issues and recognise that being truthful and honest can have a personal impact on some doctors. It is no longer seen as a weakness for a clinician to admit that they are finding things emotionally challenging. There are courses and sources of support that doctors can access to help with this. It is important that healthcare professionals are given support so they can provide the best support to patients.
What information do patients want and what do they get?
There is plenty of evidence from surveys around the world that patients generally want more information about their treatment options than they usually receive (Br J Cancer 2001, 84:48–51). There are ethical, legal and social imperatives for patients to be more active, autonomous or collaborative rather than passive in decision making, which requires providing them with sufficient information. However, studies across tumour sites over the past 20 years have shown a mismatch between the information that patients want and their preferences for decision making, and what actually occurs in practice (Ann Onc 2010, 21:114–51).
A study of information preferences in 2,331 UK cancer patients (Br J Cancer 2001, 84:48–51) showed that the overwhelming majority of patients (91%) felt they needed to know their week by week progress, with only a small proportion (9%) preferring not to know. There were similarly strong preferences for knowing about the chances of cure (95% vs 5%), about all possible treatments (94% vs 6%) and about all possible side-effects (97% vs 3%). The researchers recorded the interactions in the clinic and assessed whether patients’ pre-stated information preferences had been met. Results showed that, on the whole, they were not.
The type of decision being made influences the level of involvement that patients want. A large US study (JCO 2010, 28:4364–70) showed that if there was strong evidence for efficacy regarding the treatment a doctor was about to discuss, then they were very prepared to share control of decision making with the patient. The highest rates of patient control were seen in chemotherapy decisions, while the highest rates of physician control occurred in decisions on surgery and radiation.
There was a strong expectation that, if a discussion was about treatment of metastatic breast cancer, then patient preferences should predominate because the evidence of benefits was more modest and the potential toxicity was high. However, this expectation was not realised at all, and the study revealed low patient control and high physician control in discussions about metastatic disease. Better strategies are clearly needed to engage patients in decisions when treatment is not curative.
Another key factor underpinning decision making is whether lengthier survival is worth treatment side effects. It is important to discuss the survival benefit a patient considers worth gaining to trade off the disadvantages or harms of a treatment. Studies have suggested that patients are willing to accept very high toxicity for minimal benefit. However, much of this research is flawed, being often based on hypothetical scenarios or involving patients who have already survived treatment, which biases the findings. If there is no clear survival benefit with a particular treatment option, then information on quality of life is crucial and may influence patient preferences.
Better strategies are clearly needed to engage patients in decisions when treatment is not curative
Research has shown that cancer patients value quality of life on a par with length of life. For example, a study involving 459 patients with advanced cancer found that more than half (55%) viewed quality of life and length of life as equally important (Cancer 2008, 113: 3459–66). Just over one quarter of patients (27%) saw preservation of quality of life as being their priority, while 18% opted for length of life as their preference. Further findings showed that patients most interested in quality of life had lower cancer-related distress, while those prioritising length of life were more distressed generally and wanted more supportive and less pessimistic communication styles.
This is interesting because, if a doctor taps into the fact that the patient is very distressed and wants optimistic communication, then there is a strong risk of overemphasising the potential benefits of a treatment and underestimating the possible disadvantages.
How patients perceive messages
A recent study of 100 patients with locally advanced or metastatic cancer explored their perceptions of the compassion and trust demonstrated in two filmed doctor/patient consultation scenarios (JAMA Oncol 2015, 1:176–83). Both scenarios involved patients with advanced cancers who had received several lines of chemotherapy, had a poor performance status, and who were poor candidates for further treatment. The doctors made equal numbers of empathic statements and used similar body language in both scenarios, but the messages being conveyed differed in their level of optimism. The doctor in the first video was explicit about the lack of further options, while the doctor in the second scenario gave vague information about the possibility of some further options if the patient’s performance status improved.
The results showed that patients rated the physician’s compassion higher after watching the more optimistic video. Just over half (57%) of patients preferred the doctor delivering the more optimistic message, 21% had no preference and 22% preferred the less optimistic message. Higher perceptions of compassion were associated with greater trust in the doctor, independent of the message type. These findings demonstrate that communicating in a way that is honest but also compassionate will engender trust in patients, which is reassuring for doctors concerned that sharing difficult information will somehow lose a patient’s trust.
Question: Given that the research showed some patients preferred a more optimistic message while others preferred a less optimistic approach, is there any value in trying to determine a patient’s preference before having a consultation?
Answer: Doctors with good communication skills can usually work this out. In addition, with the exception of patients who initially present with metastatic disease, oncologists usually already know a patient with advanced cancer, and have already built up a relationship and understanding of how they prefer to receive information. An even more important issue is that one can always be optimistic and positive about situations that can potentially be improved, such as reassuring the patient that the team will manage their pain better or look for ways to increase their appetite.
Comment: It reminds me of something I was told early in my career, ‘Never tell a patient there’s nothing you can do.’
Challenges within the doctor/patient relationship
There are several challenges that affect the relationship between a doctor and patient. Healthcare policy in different countries affects the throughput of patients, potentially leading to very busy clinics, with targets and cost-containment impacting on the amount of time available to spend with each one. Patients’ expectations have a major impact on communication during consultations, particularly when they have seen the possibility of new ‘wonder drugs’ in the media. Doctors have to manage a great deal of misinformation from the media and the Internet, which can use up consultation time. Access to novel therapies can also be variable, affecting the options that may be discussed.
Patients’ expectations have a major impact on communication during consultations
Another factor now affecting the doctor/patient relationship is that most doctors now use computers to make notes during a consultation. A very interesting paper, ‘You, me and computer makes three’ (J Gen Intern Med 2015, 30:1–2), explored how the presence of a computer makes dyadic exchanges more complicated. The challenge of truth telling is a further crucial issue in effective communication between doctors and patients.
Key aspects of effective communication
Patients need more honest information about the therapeutic intent of treatment than is generally realised. Information should be delivered in a kindly, well-paced and non-patronising manner that is appropriate for the individual. The danger of failing to provide patients with sufficient information is that they then become easy prey for charlatans trying to sell treatments on the Internet.
Censoring of information
Doctors often try to ‘protect’ patients from sad and bad news, particularly regarding prognosis, based on the well-intentioned but misguided notion that what a patient does not know will not harm them.
There is an expectation that patients will ask if they want to know, which commonly they do not, and that sharing difficult news may cause them unnecessary emotional distress or make them lose hope and not enjoy the time they have left.
Thinking that a patient may lose hope if given accurate information is based on the assumption that hope is solely centred around cure and so truthful disclosure will destroy this. However, this is unethical. Preservation of unrealistic hope prevents energies being directed towards realistic, achievable goals and hopes. It is important that doctors consider whether it is ethical to encourage physically weak and exhausted patients to keep fighting for implausible outcomes.
Doctors may consider that outcomes are too difficult to predict with accuracy, so are better not discussed. Modern western cultures have a tendency to deny death and focus on new medical advances. This results in healthcare professionals and patients harbouring unrealistic expectations about the likely therapeutic benefits of modern medicine.
Failure to prognosticate is not just about unpredictability. Research suggests that the accuracy of clinicians’ predictions for prognosis is poor, with errors being almost always (90%) in an optimistic direction. There is evidence to show that the better a doctor knows a patient, in terms of length and intensity of contact, the more likely they are to overestimate survival (BMJ 2000, 320:469). These factors mean that doctors sometimes adopt ‘doing something’ behaviours rather than focusing on the honest but painful conversations that are needed.
Ensuring patients understand the benefits of treatment
When discussing new drug options with patients, it is important to remember that many have been approved based on progression-free survival (PFS) data without having demonstrated increased overall survival.
Discussions should help patients to be clear on what progression-free survival means and the therapeutic intent of the treatment they are being offered, checking their goals and priorities and the trade-off between toxicity, quality of life and survival.
A study of consultations between 32 oncologists and 90 patients with a range of metastatic cancers showed that the therapeutic aims of offering drugs that improve only PFS are generally misunderstood by patients, and oncologists may be overly optimistic about likely benefits (Support Care Cancer 2017, 25:237–44).
After consultations, only 4 of the 90 patients recalled any explanation of the therapeutic aim or PFS for the new drug treatment their oncologist had discussed with them; 57% had ‘no idea’ or were ‘unclear’ what PFS meant, 32% knew it was about ‘controlling cancer’ and 11% said it was about ‘extending life’.
From the oncologists’ perspectives, the benefits they expected with treatment often exceeded trial results. They predicted no likely benefit or uncertainty for 44/90 (49%) of patients who were nevertheless prescribed treatment. Just over half (51%) of patients said that palliative care options were not discussed with them.
There can be a mismatch between what oncologists believe they have said in a consultation and what patients believe they have heard. A study of 50 consultations found that clinicians said they discussed prognosis in half of cases (25/50) (JCO 2011, 29:61–68). However, only 12% of patients (6/50) said it was discussed. Observers of the consultations reported hearing prognosis discussed in 20% (10/50) of cases.
Question: Is there a hope from clinicians that the patient in front of them will outperform the median in terms of benefit from treatment?
Answer: That’s probably true, but the median survival comes from clinical trial data in patients fulfilling the stringent eligibility criteria, while patients in real-life clinical practice may have comorbidities
Personal and professional boundaries
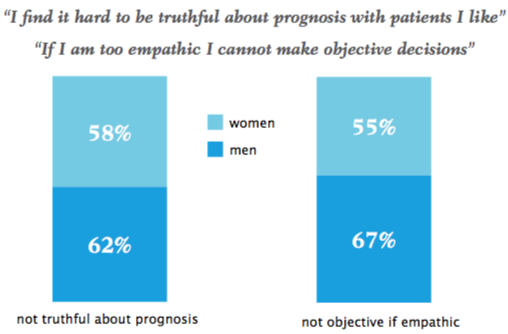
A survey of young oncologists found that many doctors feel that having an empathic relation with their patients makes it harder for them to be objective about, and communicate clearly, information that could be upsetting. Source: L Fallow eld et al (2014) Lancet Oncol 15:1423‒24
A survey of 338 young oncologists conducted in 2014 for a workshop run by the European Society for Medical Oncology showed the blurring of personal and professional boundaries (see figure ‘Personal and professional boundaries‘). Nearly two-thirds of male oncologists (62%) and 58% of female oncologists agreed with the statement, “I find it hard to be truthful about prognosis with patients I like.” Similar numbers (67% of men and 55% of women) agreed with the statement, “If I am too empathic I cannot make objective decisions” (Lancet Oncol 2014, 15:1423–24). The results illustrate how difficult doctors find it to share bad news with patients.
Early referral to palliative and supportive care services
Many data show that early referral to palliative and supportive care services benefits patients’ psychological and physical well-being and improves survival, as well as benefiting caregivers. However, doctors can find it difficult to initiate discussions about palliative care, particularly if they have close emotional bonds with the patient and their family (Support Care Cancer 2016, 24:3873–81).
Some clinicians feel it is an admission of defeat and personal failure, while others may be responding to unrealistic hopes of the patient and their family for a miracle with further anticancer treatment.
A study of 160 haematologists and oncologists taking part in 1,039 patient consultations about palliation and 1,768 consultations about active treatment or remission showed the doctors were significantly less satisfied with consultations when palliation was discussed, even when communication was good (P<0.0001) (Pall Med 2002, 16:297–303). Rating their self-confidence, doctors were more confident talking with patients about side effects of treatment (mean of 7.28 on 10-cm visual analogue scale) than telling them they have a recurrence (6.62) or that active therapy is being replaced with symptomatic care only (5.76).
Doctors can find it difficult to initiate discussions about palliative care, particularly if they have close bonds with the patient
Results from a study on the impact of the ‘Choosing Wisely’ campaign run by the American Society of Clinical Oncology (which encourages clinicians to avoid treatments not supported by evidence) showed that 71–76% of 28,731 patients aged 65 years or less, who died from metastatic cancer, were still receiving aggressive anticancer treatment within the last 30 days of life (JCO 2016, 10.1200/JCO.2016.34.18_suppl.LBA10033).
Almost one-third of the patients died in hospital, with only 14–18% receiving hospice care, suggesting substantial overuse of aggressive treatment at the end of life.
In colorectal and breast cancer, the proportion of patients treated with anticancer agents during their last month of life had remained unchanged since the campaign; in other cancers it had increased.
Optimal communication in metastatic cancer
Clinicians should start communication with advanced cancer patients with a platform of certainty about the issues that are clear and reinforce the message that many patients with metastatic disease live well with a good quality of life.
Hopefulness is important, but this should be grounded on credible, reality-based possibilities of likely prognosis with and without different treatment options. Doctors should know the data and also recognise and question their own motives for recommendations they make.
It is essential to provide positive information about the benefits of good quality supportive care, stressing that something can always be done to relieve many of the worst symptoms of advanced cancer, explaining the options for pain relief, stopping nausea and improving appetite.
There are many evidence-based courses that can help doctors to communicate in a clear, honest and empathic manner. However, there are fewer on navigating the boundaries between personal and professional involvement.
It is important to recognise that encouraging doctors to get closer to the emotional needs of patients and their families puts doctors at psychological risk and to support them with this. Doctors should also be aware of their own neediness and motives in discussing treatment options with patients, and be less nihilistic about supportive care.




This grandround was first presented by Lesley Fallowfield, from Sussex Health Outcomes Research & Education in Cancer, Brighton, UK, as a live webcast for the European School of Oncology. Richard Simcock, from Sussex Cancer Centre, Brighton, UK, poses questions raised during the presentation. It was edited by Susan Mayor. The webcast of this and other e-sessions can be accessed at e-eso.net.