The European Commission has issued a warning about a 1 million projected shortfall in Europe’s clinical workforce by 2020 – with nursing shortages accounting for more than half the total. Marc Beishon reports on the severe strains already apparent across our health systems, and looks at some policies that could help address the problem.
“We just aren’t able to spend much time with patients – we can often only talk while we put in an IV line. This has an impact on care but also on us: sometimes we don’t have time to go the toilet, our phone is always ringing, and it’s very stressful just trying to manage our daily agenda, let alone any extras. And we know that our patients need better: more time for them, more support, more activities. We have no psychological support, and patients only get it from nurses or doctors. Sometimes they just need a five-minute talk and we can’t give that to them. It is very depressing for us to know that.”
So speaks Sara Torcato Parreira, a specialist oncology nurse at Fernando Fonseca hospital, in Amadora, Portugal, a country that has been one of the worst sufferers from the Great Recession that hit Europe after the 2008 financial crash. But this snapshot is also typical of many oncology departments around Europe, where cancer services are having to cope with ever-increasing patient loads due to ageing populations and longer survival times, while health budgets are failing to keep up, or in some cases are being cut.
A report by the European Observatory on Health Systems and Policies – ‘Economic crisis, health systems and health in Europe: impact and implications for policy’ – noted that the crisis radically changed the focus from “worrying about how to pay for healthcare in 30 years’ time to how to pay for it in the next three months”. Not all European countries have been badly affected, but the report notes that in Croatia, Greece, Ireland, Latvia and Portugal, public spending on health was actually lower in 2012 than in 2007.
Nurses are particularly feeling the strain. In the EU as a whole, their numbers have been increasing at around half the rate of doctors’ for the best part of 15 years. In central and eastern European countries, the nursing workforce has barely increased at all over the last 25 years. As the frontline workforce vital to all aspects of care throughout the patient journey, it is easy to understand why many of them feel they are reaching breaking point, and worry that patient care is suffering.
Lemme-Liis Aruvali, a young nurse at the Haematology-Oncology Clinic in Tartu, Estonia, says: “Our patients don’t get enough time with the doctors or nurses to ask questions and discuss problems. Doctors are overworking and nurses who work with outpatients or inpatients are often also too busy. Patients may not get as much time and attention as they need, so they may be more confused, scared and unaware.”
And in Slovenia, Katarina Lokar, formerly head nurse at Ljubljana’s Institute of Oncology, who now works in epidemiology and cancer registration, reports similar concerns over the capacity shortage in Slovenia. “We are having to deal with a shortage of nurses and doctors, as well as of other professional and supporting staff. We have had a very hard time in the last four years due to the economic crisis and budgetary restrictions. There are big problems with long waiting times for some treatments, including in oncology. This means full waiting rooms, and a lot of people with bad immune systems in closed spaces, and the risk of transfer of hospital infections, as well as less time for holistic care. Psychosocial care is often viewed as less important than getting the treatment on time.”
The shortages of staff and pressures on the remaining workforce are not confined to smaller, less well-off countries. In the UK, a country that is still playing ‘catch-up’ with better performing peers in Europe, and where waiting times for suspected cancer and first treatment have worsened in the past few years, an independent report identifies problems in the numbers and configuration of the cancer workforce as critical issues in delivering better care.
A report carried out by an independent cancer taskforce, ‘Achieving world-class outcomes: a strategy for England 2015–2020’, notes “significant workforce deficits, particularly in diagnostic services, oncology, and in specialist nursing support,” which it claims “result in severe bottlenecks in the diagnostic process, suboptimal care in certain parts of the country, and an inability to deliver newer, evidence-based and cost-effective treatments.”
“This means full waiting rooms, and a lot of people with badimmune systems
in closed spaces, as well as less time for holistic care”
The report also highlights the needs of a growing number of people with chronic cancer conditions who need to be cared for in the community by a combination of health and social services, and says the system lacks the capacity, and has the wrong workforce configuration to support patients beyond their initial treatment.
Common problems
Healthcare systems are hard to compare, but all countries are facing increasing numbers of people, especially older people, living with cancer; new, costly and complex treatments such as immunotherapies; and difficulties in attracting young health professionals to take up positions such as primary care practitioners, amid an overall trend for doctors to be older with not enough people in training or being recruited in some countries.
Several countries are also increasing funding for primary care,
aiming to shift care out of hospitals to the community
There are several policy responses that countries are using to try to stabilise their health systems and help protect those hardest hit, such as vulnerable and unemployed people, including raising taxes, introducing user charges for some, and restructuring purchasing systems to cut the price of buying drugs and other products and services. But several countries are also increasing funding for primary care, aiming to shift care out of hospitals to the community, as there is evidence that health systems with strong primary care perform better.
So the economic crisis may have stimulated much needed changes, and as many as 15 countries are reported to have taken steps to shift care out of hospitals. There also appears to have been a speeding up of closures and mergers of hospitals in the acute sector. In turn, though, this is raising questions about the availability of staff with the appropriate skills to work in expanded community settings, such as GPs and nur-ses with specialist knowledge in chronic conditions such as cancer. This has been a particular problem in countries where the numbers and pay of health professionals have been cut, which includes many of the countries subject to the ‘economic adjustment programmes’ determined by the European Union and International Monetary Fund, such as Greece, Ireland and Portugal.
Salaries and conditions for staff are currently not sufficient
to stem a substantial brain drain
Europe-wide data are not easy to come by, at least in terms of staffing shortages. Such research as has been done seems to indicate that the staffing situation is much less of a problem for doctors than nurses, at least in oncology. In medical oncology, a paper titled ‘The landscape of medical oncology in Europe by 2020’ (Ann Oncol 2014, 25: 525–8) found that the availability of oncologists will probably meet the projected need in most of the 12 countries analysed, provided that current increases in doctor numbers continues (the mean increase was a healthy 5% a year), and that there are no unforeseen changes in cancer incidence. The authors do note, though, that little information was available from eastern European countries.
In Romania, Laura Mazilu, head of oncology at Constanta Emergency Hospital, says there are shortages of oncologists and nurses in her country, although her own department has loyal staff. “We don’t currently have a recruitment problem, but we are only a small 25-bed oncology department,” she says. “We are though overloaded with patients.”
“We have a shortage of nurses more than doctors,
especially specialist nurses”
Funding is a big problem in Romania, which has been spending only about 5% of its GDP on healthcare, and salaries and conditions for staff are currently not sufficient to stem a substantial brain drain to other countries, and also to the private sector in clinics in the capital, Bucharest.
Mazilu says that while her team in Constanta – the country’s fifth largest city – is able to provide a good standard of medical oncology care, according to international guidelines, the hospital currently lacks a radiotherapy unit. “The ‘bunker’ is there but not the staff or machinery, so patients have to travel to other centres,” she says, adding that they also lack specialist palliative and psychosocial care professionals.
The staffing situation is far worse in rural areas (Feraru, Global J Med Res Interdisc 2013, 13(5)). As reported on thecancerblog.net, the county hospital in Vaslui, along Romania’s eastern border, caters for a population of 375,000, but has no oncologist at all; in the west of the country, one oncologist based in Resita has responsibility for over 8,000 patients recorded in the cancer registry.
EU recognition of medical oncology as a medical specialism in 2011 – a longstanding demand of the European Society for Medical Oncology (ESMO) – will have helped encourage young doctors into the field, but may also have added to the challenges poorer countries like Romania face in retaining their trained specialists. ESMO has set up a ‘women for oncology’ committee to look at leadership and work–life balance issues – many countries still suffer from male-dominated hierarchies.
The European Society of Surgical Oncology is now looking to promote a similar harmonisation of minimum training and competencies required for all surgeons who treat cancer patients, with its recently published Global Curriculum for Surgical Oncology, which has, as its principal aim, raising standards in cancer surgery. And ESTRO, the society of radiotherapists, has recently published the latest paper in its Health Economics in Radiation Oncology (HERO) project, in which it predicts a 16% increase in the number of radiation treatment courses will be needed from 2012 to 2025, varying from 5% to 30% across Europe, which will require some increases in staffing capacity among radiotherapists and the many other specialities required to plan and deliver the treatment.
Clearly, the workforce is also only one part of establishing high-quality cancer care – quality systems, research and technology are all critical, and the drive for quality can also have a big impact on the location and size of cancer centres. There is plenty to investigate in how multidisciplinary teams and information technology, including telemedicine, can best be configured for various tumour types and patient pathways.
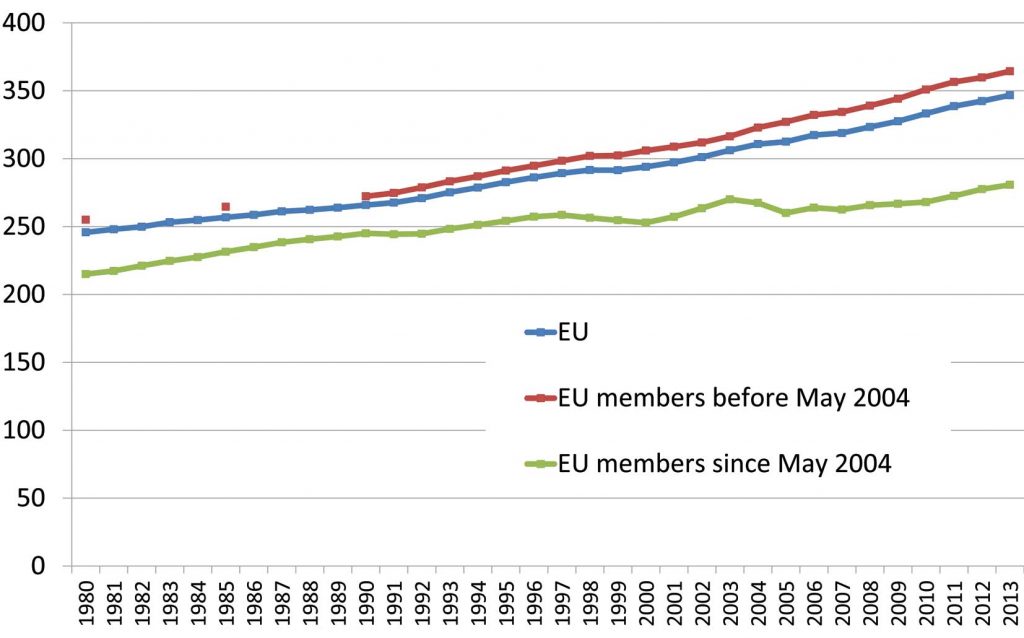
Growth trends in the EU healthcare workforce
Physicians/100,000 population
Nurses/100,000 population
The number of doctors per head of population rose by almost 20% between 2000 and 2013 – though more slowly in central and eastern European countries. The number of nurses rose at less than half that rate over the same period, remaining static in most of central and eastern Europe. The proportion of Europe’s population aged over 65 years has more than doubled over the same period.
Sources: Improving the Skills Mix for Chronic Care in Europe: Presentation by Matthias Wismar, European Observatory on Health Systems and Policies http://ec.europa.eu/health/workforce/docs/ev_20151116_co06_en.pdf (accessed 14 November 2016); Eurostat
There are also gaps in technical positions, such as in nuclear medicine and radiotherapy, and a need to invest more in diagnostic services. The NHS in the UK, for example, is aiming to have sufficient numbers of sonographers, radiographers and radiologists in the cancer workforce, and will train 200 more ‘non-medical’ endoscopists by 2018 for gastrointestinal investigations – non-medical meaning ‘not doctors’, but nurses and other professionals. Currently, one in ten consultant posts in breast radiology and 15% of radiographer jobs are unfilled in the NHS.
Pressure on the frontline
The cancer nursing workforce has probably attracted the most attention, as it has a big impact on patients. ECCO, the European Cancer Organisation, last year made nursing one of its top ‘oncopolicy’ issues, and has kicked off a nursing project, which has greatly pleased Daniel Kelly, president of the European Oncology Nursing Society (EONS).
“The truth is we are not heard by politicians until something bad happens”
Of all the jobs involved with cancer, nursing has greatest variation across Europe, says Kelly, who is a professor of nursing research at Cardiff University in Wales. “Some countries are open to innovative ideas on how nurses can take on much more than they traditionally did, but others still have an old-fashioned picture and restrict the roles of nurses,” he says.
Countries such as the UK, Sweden and Ireland have had advanced and specialist cancer nursing roles in place for some time, he notes – but sustaining and developing such roles needs support. Helena Ullgren, who coordinates ‘contact’ nurses from the Karolinska University Hospital in Stockholm, says all patients are entitled to have a contact nurse who specialises in one or two cancers (her own interest is head and neck cancer). “But we have a shortage of nurses, more so than doctors, and in particular these specialist nurses. We don’t offer high enough salaries, there are heavy workloads and, especially, we don’t offer good career paths – so we have a high nurse turnover,” she says. “Nurses want to know they can train to be a specialist or take a Masters course, and the university has places for them, but employers are reluctant to let them attend owing to staff shortages.”
To make things worse, says Ullgren, some hospitals are now placing generalist nurses in specialist cancer or surgical care roles, without recognition of the specialist status of these posts, and the Swedish National Board of Health and Welfare no longer issues licences for such positions. “This undermines the system for everyone – we have gone backwards in Sweden,” says Ullgren.
Cancer outcomes are currently good though, and patients are mostly satisfied with their care, she adds. But there is concern about workloads and staff working in ‘silos’: “We feel that patient safety is getting worse, which can happen without timely handovers of patients between departments, for example. When you have limited time you tend to work in silos, and many of us feel we cannot influence our daily working conditions, as decision-making is too hierarchical. Hospitals need to empower their staff much more.”
The risk posed to patients by using nurses to take on roles they are neither adequately trained nor recognised for is something that also concerns Katarina Lokar in Slovenia. “At the Institute of Oncology, nurses in the outpatient unit also prepare cytotoxic drugs – the pharmacy covers only hospital wards – and this is more than half of all drugs, and the standards are lower than in the pharmacy. This brings a number of safety issues and additional workload.”
She adds that they lack staff, funding, specialised knowledge, facil-ities and equipment, and says that patients should expect better. “Mostly we have understanding patients who are willing to wait, because they see how much work is done and how many patients there are. In my opinion they are too good with us – I think they should be more demanding. The truth is that we [nurses and doctors and other professionals and management] are not heard by the politicians unless something bad happens.”
Parreira in Portugal says there is a freeze on hiring more health professionals. In her department, which has eight nurses, she is the only cancer nurse specialist, and someone who wants more qualifications has to use their own time and money to do so. “The primary care system suffers from a similar lack of resources – there are plans to have a network of community nurses, in particular for palliative care, though.” One barrier comes not from the authorities but from doctors – despite being short staffed, they have been against nurse specialists taking on initial assessments in emergency departments, she says.
Offering better training and recognition for specialist cancer nurses may prove key to solving some countries’ healthcare staffing problems, according to researchers behind the EU-funded project which studied breast cancer roles in Scotland. The MUNROS study into the ‘Impact on practice, outcomes and cost of new roles for health professionals’, found that career progression is a primary motivating factor for nurses, which echoes the point made by Ullgren in Stockholm.
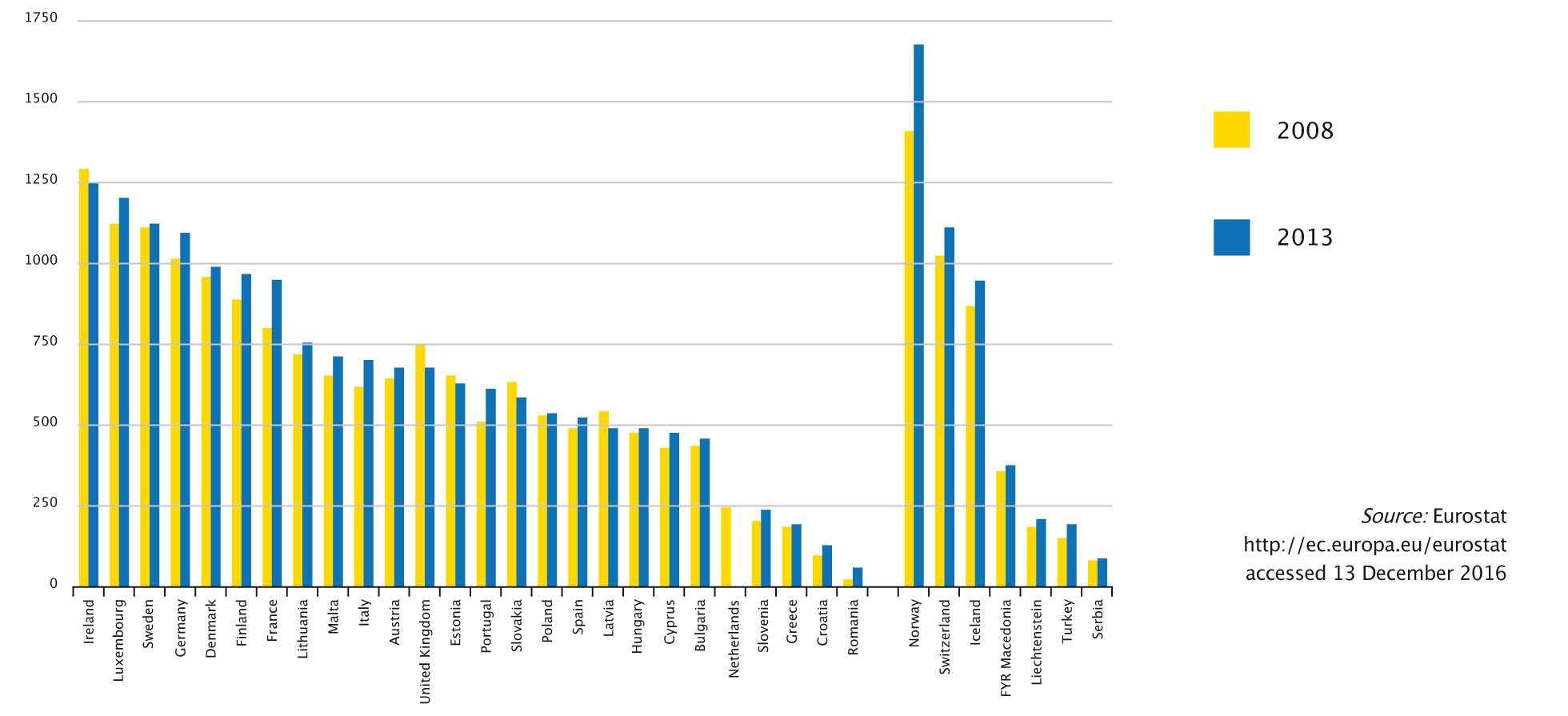
Practising nursing professionals per 100,000 population, 2008–2013
Source: Eurostat http://ec.europa.eu/eurostat accessed 13 December 2016 (click to enlarge image)
Staffing shortages are more acute in some European countries than others, with EU regulations making it easy for health professionals to travel to where job opportunities, pay and career prospects are most attractive
Some countries currently do not have any oncology nursing programmes. Lemme-Liis Aruvali says her country, Estonia, is one of them. “In Estonia we don’t have a special educational programme for oncology nurses. All nurses who work in our department are registered nurses, or students who are becoming one. We learn everything from older colleagues. We definitely need a programme for cancer nurses,” she says. The situation is similar in Slovenia. Lokar mentions attempts to introduce a national cancer nurse specialisation programme, but says it lacks financial backing for implementation, and as it is not pitched at a Master’s level, it does not meet the criteria set by European Specialist Nurses Organisations (ESNO).
“Cancer hospitals need to restrict their role to care of the acutely ill”
Some larger, more affluent, countries are also lagging. In Germany, nursing roles mostly remain at diploma level: just 5% of the nursing workforce have university degrees, and there are fewer specialist cancer nurses than in other countries, says Patrick Jahn, an oncology nurse and head of nursing research at Halle University Hospital, near Leipzig. Only about 20% of nurses in cancer centres have post-hoc basic training in procedures such as administering chemotherapy, he says, and generally at federal level the role of nursing in Germany’s national cancer plan has not been given enough emphasis. The regional government structure does not help, he adds. Things may be set to change, though: Jahn is currently sitting on an expert commission that is charged with spending over €800 million to improve the nursing situation and address a general shortage of nurses across the country.
An increased role for primary care
Where Germany does have a potential head-start is in local outpatient clinics, which Jahn explains are separate from day clinics at hospitals, and where some doctors specialised in cancer collaborate with GPs. This does make the health system more complicated, but can create stronger networks of care, he says. “But what is missing are advanced practice nurses – most of the other workers at these clinics are doctors’ assistants. We need nurses to help patients adhere to drugs and manage side effects, such as new ones we are seeing with oral targeted therapies, and provide supportive care.”
Safety concerns. When time is short, communication can suffer, for instance at handover time, leading to potentially serious mistakes
His own research is addressing the nursing role in supportive cancer care, and he further points to a trial currently underway in Hamburg, where nurses are helping patients with the side effects of oral cancer drugs to see if it improves their quality of life.
The general direction of travel, albeit a slow one at present, is for more community-based specialists and ‘blended’ roles, with people having two or more main tasks. As Kelly says, cancer hospitals need to restrict their role to care of the acutely ill, including those who present as emergency cancer cases, and those who pose particular challenges for the oncology workforce. Most cancer care should take place at home or at a day clinic, he argues.
Rebalancing care for survivors away from oncology centres and towards community/primary care is seen as a particular priority, given the rapid increase in people who are either surviving with no detectable cancer, or simply living longer with chronic disease. Recently, Macmillan reported a study showing that 7,000 colorectal cancer survivors in the UK are struggling with side effects and distress years after their diagnosis.
Other professions, such as social care, are expected
to become increasingly involved in new models of cancer care
Pilot studies run by the UK National Survivorship Initiative have shown that many survivors – particularly those with a good prognosis – are amenable to having responsibility for their care shifted to a primary care setting, and to taking a more active role in self-managing ongoing health problems.
But the same research also showed that cancer survivors will be more likely to self-manage if they are better supported with information and specialist support after their anti-cancer treatment – which is typically a role for specialist cancer nurses.
In France a project in the Auvergne region has nurses coordinating care after hospital discharge, and a greater role for GPs in caring for survivors. Getting lines of communication right between GPs and oncology specialists will be important to making this work. In Israel, the Israel Cancer Association supports GPs with annual seminars focused on topics they request. It also publishes a journal for GPs. In Stockholm, meanwhile, Ullgren says there is a new cancer rehabilitation centre that caters for long-term effects, but already an emerging issue is lack of communication with other professionals, such as palliative care nurses.
Ultimately, however, the critical shortfall in health professional staff is unlikely to be resolved by shifting roles and responsibilities between different elements of the workforce.
Other professions, such as social care, are expected to become increasingly involved in new models of cancer care, raising further issues of training, competencies and coordination. For a model of holistic support at European level, the European Commission Expert Group on Rare Diseases has recently adopted recommendations on how social services can help support people with rare diseases, such as certain cancers – see the INNOVCare project on the EURODIS rare disease group’s website.
Given the importance of care at home and in the community, there is another part of the cancer workforce that is widely neglected but which saves countries millions of euros a year – namely carers of people with cancer. Better social and financial support – and also training, given that carers often help with clinical work – for this large number of people is long overdue.




 The shortages of staff and pressures on the remaining workforce are not confined to smaller, less well-off countries. In the UK, a country that is still playing ‘catch-up’ with better performing peers in Europe, and where waiting times for suspected cancer and first treatment have worsened in the past few years, an independent report identifies problems in the numbers and configuration of the cancer workforce as critical issues in delivering better care.
The shortages of staff and pressures on the remaining workforce are not confined to smaller, less well-off countries. In the UK, a country that is still playing ‘catch-up’ with better performing peers in Europe, and where waiting times for suspected cancer and first treatment have worsened in the past few years, an independent report identifies problems in the numbers and configuration of the cancer workforce as critical issues in delivering better care. The number of doctors per head of population rose by almost 20% between 2000 and 2013 – though more slowly in central and eastern European countries. The number of nurses rose at less than half that rate over the same period, remaining static in most of central and eastern Europe. The proportion of Europe’s population aged over 65 years has more than doubled over the same period.