Combining the complementary approaches of HPV vaccination and screening could accelerate declines in the burden of cervical cancer argue Xavier Bosch and colleagues. They are proposing the HPV-FASTER protocol as a way to achieve it.
Cervical cancer is the third most common cancer in women worldwide. The burden varies widely between countries, which is largely attributed to variations in cancer prevention efforts and healthcare resources. Countries with a well-organised screening programme and high levels of participation in screening have observed a substantial decrease in cervical cancer incidence. Social inequity and access to evidence-based preventive services are major issues in cervical cancer control.
Current strategies for preventing cervical cancer include primary prevention via HPV (human papillomavirus) vaccination and secondary prevention using cytology tests or HPV detection methods to screen for cervical cancer precursors.
Cervical screening
Cytology-based screening programmes have achieved large reductions in cervical cancer incidence and mortality, particularly in countries where coverage of the target population has been at a consistently high level for more than a decade.
One limitation of cytology-based screening is its relatively low sensitivity for detecting precursor cervical cancer lesions (CIN2+) compared with HPV testing, necessitating repeated screening and complex infrastructures. These limitations are factors behind the failure to successfully implement cervical cytology screening in most developing countries, where screening tends to be unorganised and selective for individuals from high socioeconomic classes in urban areas (Vaccine 2012, 30 Suppl 5: F183–191).
Clinical trials have shown that HPV testing provides a 30–40% gain in sensitivity for detecting precursor lesions of cervical cancer (CIN2+ and CIN3+) compared to cytology, at the cost of a 3–5% loss in specificity. HPV testing also shows less variability across populations (Int J Cancer 2014, 134:1835–43).
Likewise, previous HPV-negative tests predict a lower incidence of subsequent detection of CIN3+, as compared to a previous normal cytology screening result, thereby allowing safe extension of the intervals between screening episodes.
Reviews have concluded that HPV-based technologies could be used for primary screening (Ann Oncol 2014, 25:927–35), with several guidelines currently recommending HPV testing for primary screening.
However, since an increase in overdiagnosis of naturally regressive CIN is observed in women below the age of 30, the World Health Organization mainly recommends HPV-based screening in women over 30 years old (over 25 years in some protocols).
In order to be effective at population levels, screening initiatives need the infrastructure of publicly funded, coordinated and centralised programmes, with networks of specialised colposcopy clinics to ensure proper management of positive screens.
Desired features include ‘call and recall’ procedures, regular staff training, and systematic audits of invasive cancer cases occurring within screened populations.
The logistics and technology needed for successful deployment remain barriers to the introduction and sustainability of cervical screening in low-income countries.
HPV vaccines
At present three prophylactic HPV vaccines are licensed – the tetravalent vaccine Gardasil, based on virus-like particle (VLP) antigens for HPV types 6, 11, 16, and 18; the bivalent vaccine Cervarix, based on VLP antigens for HPV types 16 and 18; and a nonavalent vaccine Gardasil9, based on VLP antigens for HPV types 6, 11, 16, 18, 31, 33, 45, 52 and 58.
HPV vaccination programmes mainly target single cohorts of adolescent girls (aged 9–14 years), with some countries extending the coverage up to age 18 or 26. However, women above the age of 25 are also vulnerable to new infections. Recent results of phase III HPV vaccination trials have documented that the vaccine is highly effective at preventing HPV-specific persistent infection and CIN1+ in adult women testing DNA-negative for HPV (some 85–95% of women in screening age groups), with efficacy estimates above 80%.
The vaccination scenario is rapidly changing with the arrival of the 9vHPV vaccine, which is expected to protect against 95–100% of HPV infections included in the vaccine, which account for some 80% of CIN2+ lesions and 90% of invasive cervical cancers worldwide.
Further, in countries that have implemented HPV vaccination programmes, a significant reduction of prevalent infections, precancerous lesions and genital warts has been observed in the vaccinated cohorts, and also in their sexual partners, demonstrating the effectiveness of HPV vaccination, including a herd-protection effect (Clin Ther 2014: 17:23).
The cervical cancer prevention field is now expanding in three ways. The age group for vaccination is expanding, by reducing the vaccination age towards paediatric populations
(age 9+), and increasing the upper limit to include young women (e.g. up to age 26 in Australia and Denmark). Boys are being included in routine vaccination programmes (e.g. up to age 18 in Australia and Finland). And HPV DNA testing is being used for primary screening.
The HPV-FASTER protocol
The HPV-FASTER protocol has been developed to address disconnects between HPV screening and vaccination, through combining both strategies with the aim of accelerating reductions in cervical cancer incidence and mortality.
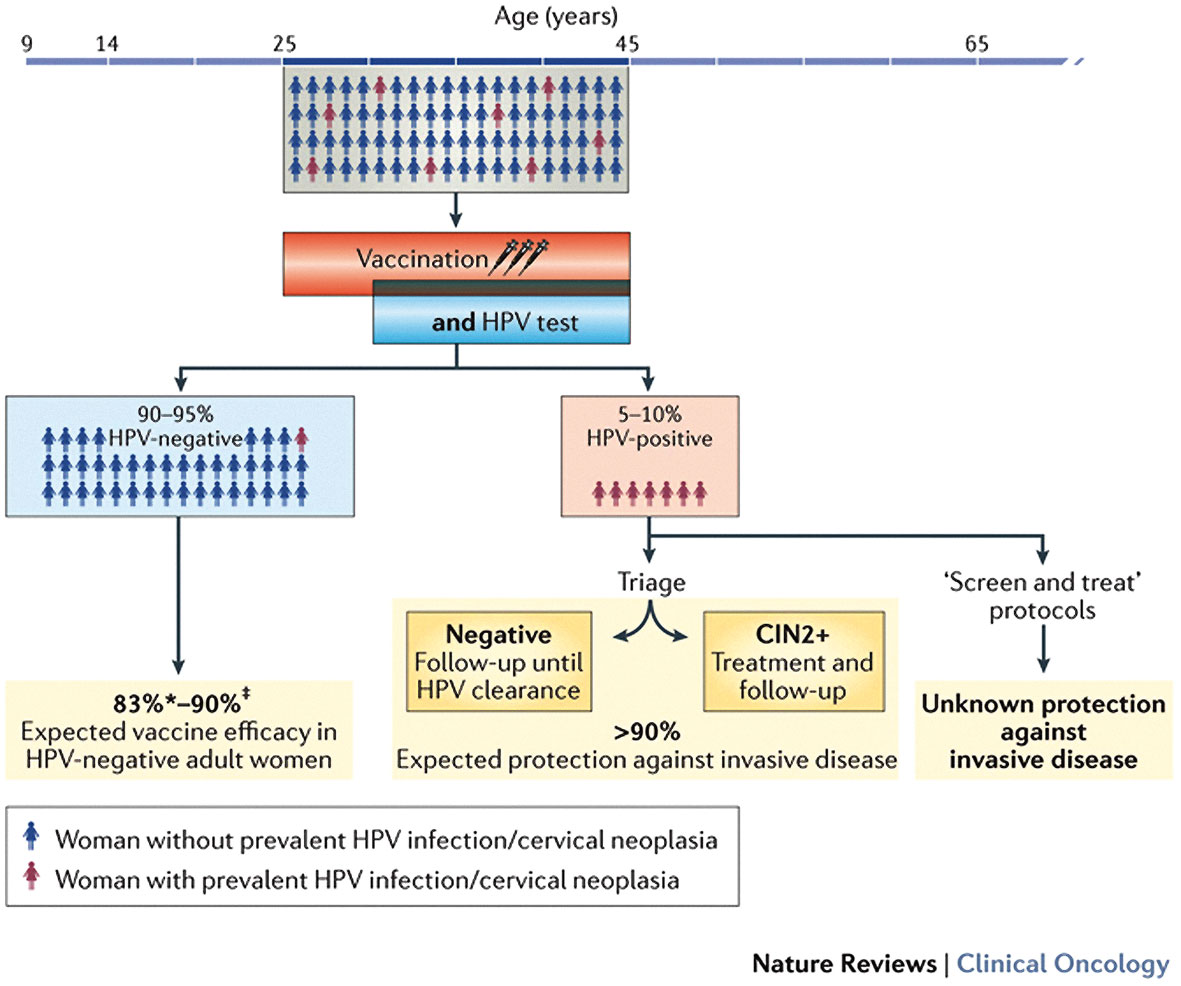
The concept proposes a generalised HPV vaccination campaign aimed at females aged from 9 up to 30–45 years, paired with at least one HPV-screening test at any age above 30 years, and triage/diagnostic assessments of women who screen HPV positive (see figure).
The HPV-FASTER core concept
(click to enlarge)
The HPV-FASTER strategy proposes to offer HPV vaccination to women aged 25–45 years, with concomitant HPV-DNA screening in women aged 30 years and above. Additional research will have to determine the required number of HPV-screening events in the vaccinated individuals and the optimal sensitivity of the HPV tests adopted, in order to maximise cervical cancer prevention. Updated results on HPV-vaccine studies, notably on efficacy, duration of protection, and spectrum of HPV genotypes covered, are expected to significantly reshape the quantitative predictions for prevention of the future HPV-FASTER protocols.
CIN2+ – cervical intraepithelial neoplasia grade 2 or higher; HPV – human papillomavirus.
One controversial element of the HPV-FASTER strategy is whether to vaccinate women irrespective of their HPV status, or restrict vaccination to women who test HPV-DNA negative. Current HPV vaccines lack therapeutic effects against development of cervical lesions in women who are HPV-DNA positive (JAMA 2007, 298:743–53).
Evidence indicates that vaccination of women who are HPV-positive or CIN2+ does not interfere with treatment or follow-up of CIN2+. Compliance with three-dose vacci-nation regimens, it is felt, would be facilitated if first doses were delivered in combination with the HPV test in women aged over 30 years. One HPV-based screen after vaccination would identify most of the CIN2+ cases and HPV positive women requiring more frequent follow-up.
An alternative HPV-FASTER protocol could be to vaccinate females aged 9 to 45 years, and offer HPV screening at any age above 30 years, but starting at one to five years after vaccination, rather than at the time of the first dose. For effectiveness, it is of great importance for HPV-FASTER to ensure all women are HPV tested at least once after vaccination, as no protection is available against current infections.
Finally, the most conservative HPV-FASTER approach, based on women who are HPV-positive being at low risk of invasive disease if triaged, offers vaccination only to women testing HPV-negative up to 45 years.
Implementation and research
With HPV-FASTER, cervical cancer prevention models would evolve from traditional ‘repeated screening rounds’ to a simplified ‘screen and vaccine’ strategy, followed by campaigns of generalised HPV vaccination of girls aged 9–14. The approach would allow screening to remain more intensive for pockets of non-vaccinated adult women, marginal social subgroups and immigrant populations who might have missed routine vaccination.
The HPV-FASTER trials will address several important questions such as:
Which is the best lifetime combination of screening and vaccination for women in all age groups?
Which combination will offer a more favourable cost–benefit balance without compromising security under limited budgetary resources?
How can we bridge the inequality gaps displayed in the incidence and mortality rates across countries?
How can we coordinate the screening and the vaccination programmes in any given country, which are typically separated in national budgets, composition of their advisory boards, and logistics in daily practice?
Optimal combinations of vaccination and screening would be different in countries where minimal screening activities are in place compared with those where screening is established.
Uncertainties regarding HPV-FASTER
Uncertainties for HPV-FASTER include whether HPV infections that occur after 30 years are an important cause of cervical cancer, and whether women who have cleared HPV infections and test HPV-DNA negative are susceptible to new infections with the same or other types of HPV.
There are also questions about the level of continuing participation in reduced follow-up (e.g. five screening events over a lifetime), if programmes create a false sense of complete protection.
Finally, in developing countries, HPV screening and associated triage/treatment need to be sustainable in local settings. Where vaccination campaigns and one round of HPV screening/ treatment might be too costly, decisions will need to be made regarding which preventive measure should be introduced first.
Modelling cost-effectiveness
Natural history models of HPV and cervical cancer will be used to estimate the cost-effectiveness of different strategies and variants of the HPV-FASTER design. In terms of effectiveness, several model-based studies have predicted that catch-up vaccination campaigns of older girls and young women would advance by several years the impact of HPV vaccination on cancer reduction compared to vaccinating only adolescent girls (Int J Public Health 2011, 56:153–62).
In terms of cost-effectiveness, all studies show the same decreasing pattern with advanced age at first vaccination, but they are not consistent regarding the age at which vaccination becomes unattractive.
The price of the vaccine has a major impact on the cost-effectiveness balance in the models. As an example, when the vaccine price is reduced from €€105 to €€45 per dose, the age limit for cost-effectiveness (under US parameters) changes from 12-year-old girls to 30-year-old women (J Infect Dis 2011, 204:377–84).
These results suggest that systematic HPV vaccination of women up to the age of 30 years – and possibly up to the ages of 40–45 years – at a sustainable price, paired with a limited number of lifetime HPV screening visits, could be clinically effective and cost-effective in many settings.
Ongoing studies
In Europe, the European Commission funded CoheaHr, a feasibility project across 11 countries, to address social and logistic uncertainties regarding HPV-FASTER.
If the initial evaluation proves successful, the aim is to organise a full-scale trial randomly assigning women aged 25–45 years to HPV screening or HPV screening plus HPV vaccination, with endpoints including incidence rates of HPV infections and cervical pre-neoplastic lesions.
In Mexico, the FRIDA trial is offering HPV testing and HPV16/18 genotyping to large numbers of women aged 25 to 75 years who have limited access to screening. To examine gains from HPV vaccination, the FRIDA-2 trial will compare repeated HPV screening with repeated screening and vaccination, with the trial powered to examine protection gains in the 25–55-year age group. Other researchers are exploring opportunities to implement the HPV-FASTER concept in settings with no or minimal screening activities in place, such as Latin America, in under-screened aboriginal populations in Australia, and in other isolated populations.
Conclusions
The successful combinations of HPV screening / treatment and HPV vaccination has the potential to move the preventive paradigm from our current ‘cancer control’ objective to a cervical ‘cancer elimination’ goal in selected populations – an essential step to envision cancer eradication in the future.
Xavier Bosch is a senior consultant at the Cancer Epidemiology Research Programme, at the Catalan Institute of Oncology, L’Hospitalet de Llobregat, in Barcelona.
Take home message from the author
“Since the introduction of HPV vaccines in 2006 significant advances have been made, notably showing very high protection and safety among adult women, provided they are HPV-negative at the time of vaccination (i.e. no therapeutic effect). Likewise, more than 20 clinical trials have shown very good sensitivity to detecting HPV-positive cases in the context of screening programmes. Yet the field of cervical cancer prevention is still based on the limited use of HPV vaccines and repeated screening tests (cytology in most countries and HPV tests in some). Most international regulations and guidelines (including the EU’s) recommend HPV tests as the single test for primary screening at longer intervals (i.e. 5+ years), and starting not before age 30. Only a few countries, such as Australia, support vaccination programmes that extend recommendations for vaccination to age 26 years.
Open questions
The two alternatives for HPV-screened women are to undergo repeat HPV tests every five years, or to receive a broad spectrum vaccine and then perhaps one or two lifetime additional tests. The number of lifetime additional tests will need to be determined by trials, but in reality the number of tests undertaken in developing countries is likely to be very small. Middle-aged women who are HPV-positive will need to be triaged and treated if necessary.
HPV-FASTER
The HPV-FASTER alternative calls for generalised vaccination of girls and young women (i.e. from age 9 to 45), paired with at least one episode of HPV screening from ages 25/30 to 65. HPV vaccination of young women would be offered at enrolment irrespective of their HPV status. The HPV-FASTER alternative is anticipated to be a cost-effective option in developed countries with generalised social access to quality-monitored screening services. More important, the HPV-FASTER alternative is proposed as a game changer for countries with historically high cervical cancer incidence rates, limited screening deployment, but good vaccination expertise, such as the Latin American region and Eastern Europe.
Further studies
We are organising formal trials comparing HPV screening and vaccination against HPV screening alone. In countries with limited resources (where there is one screening episode at around age 30), projects will need to be put in place to monitor vaccination coverage, quality of treatment of women who test HPV positive, and long-term incidence of cervical cancer.




This is an abridged version of FX Bosch et al (2016) HPV-FASTER: broadening the scope for prevention of HPV-related cancer. Nat Rev Clin Oncol 13:119–132. It was edited by Janet Fricker and is published with permission