With increasing numbers of cancer drugs being approved on shorter trials that involve fewer patients, getting accurate reports of adverse events and side effects after approval is increasingly important. Maria Delaney reports on efforts to encourage us all to be alert for – and report – possible side effects from the medications we take.
Have you ever suffered a side effect while taking medication? Ranging from mild to severe, the majority of us have experienced some type of side effect. If so, what did you do about it? Hope that it would pass, shrug it off, notify your doctor, stop your medication…
Side effects are a common reality for patients on cancer therapies and they can often be very severe. Despite this, new studies show that they are under-reported by physicians in clinical trials, by as much as 74% for some toxicities.
And it isn’t only physicians who under-report. Gilliosa Spurrier-Bernard, melanoma advocate from Melanome-france, says that getting patients to report side effects during a clinical trial is quite hard, as they are terrified they will lose their place on the trial. She says this “is bad for pharmacovigilance after the trial, when the drugs go out into normal practice.”
As more innovative targeted therapies move from trials to the general market, continued reporting of side effects is something that some members of the oncology community are striving to improve. One way they are doing this is by putting power in the hands of patients: side effects can now be directly reported to pharmacovigilance centres in each country across the EU.
But is this direct reporting actually happening, what are the benefits, and how can it be improved?
Progress in pharmacovigilance
Pharmacovigilance has developed substantially since the initial WHO pilot Program for International Drug Monitoring was set up in the early 1960s, following the thalidomide disaster, according to Rebecca Chandler, from the Uppsala Monitoring Centre – the WHO Collaborating Centre for International Drug Monitoring, based in Sweden. “We thought it was very important to set up a network of countries so that [events] that might be occurring on a rather small level in individual countries might be seen better from a global perspective.”
“Doctors will dismiss fatigue, because they don’t know what to do with it, whereas for the patient it’s very important”
The initial 10 pilot countries has now expanded to 125 participants, with over 14 million adverse event reports collected. These reports are entered into the Monitoring Centre’s VigiBase database. As Chandler explains, there is much overlap with the data gathered by the US regulatory body, the FDA, with their reports making up approximately 50% of the entire database. This is due in part to a large number of reports collected by drug companies with headquarters in the US.
“In the United States, people often report to the drug company first, but Europe is different, with patients in individual countries reporting directly to the national pharmacovigilance centres,” says Chandler, though she adds that, in Europe, the option to report to either the company or national pharmacovigilance centres is there for both patients and physicians. The Uppsala Monitoring Centre does not collect reports directly from patients, but it would like to see more patient reporting done at a local level.
Direct reporting by patients to local pharmacovigilance authorities was first introduced by Denmark and the Netherlands in 2003. Today it should be possible for patients in all EU countries, as EU Pharmacovigilance legislation passed in 2012 requires all national centres in Europe to have a system that can receive reports directly from patients, says Chandler. In spite of this new requirement, it is still difficult for patients to report side effects in some countries due, for instance, to forms not being set up for online completion, or being simply too complex.
Outside the EU, there are many countries that have no option for patients to directly report side effects. A recent study found that patients were not allowed to report in 34 countries, or 24% of the National Competent Authorities surveyed.
Patient vs doctor reporting
Patient reporting without the influence of a healthcare professional is important, as “we know doctors underestimate certain side effects and overestimate others in terms of importance or relevance to a patient,” says patient advocate Spurrier-Bernard. “Doctors will categorically dismiss fatigue because they don’t really know what to do with it, whereas for the patient it’s very important.”
Even when side effects are reported, there are differences in how doctors and patients report them. A 2014 study found that patients’ reports are more focused on the subjective impact of the adverse event, whereas reports from health professionals include a lot of clinical information, but less on the experience of the patient.
Francesco Perrone, director of the clinical trials unit at the National Cancer Institute of Naples, has studied the difference between doctor and patient reporting in a clinical trial setting, and has found that under-reporting of toxicities in anticancer treatments by physicians ranged from 40.7% to 74.4%. He thinks the reasons for this include not having the time to talk to patients about side effects, patients being afraid to lose treatment, and not noticing side effects such as hair loss in male patients.
This leads to a problem for drugs now on the market, as there is a lack of clear knowledge of the side effects of a new drug or treatment strategy. Perrone feels “there is a high probability that the patient will be misinformed” in clinical practice, as all the side effects will not be mentioned in studies of the drug.
Spurrier-Bernard says this happens a lot from her experience in the melanoma patient group. Doctors tell patients that certain side effects are ‘nothing to do with this drug’, but “we know that these drugs are new and the doctors themselves don’t know all the side effects.”
Chandler agrees, and says that this is often due to the nature of precision medicine dividing patients into specific genetic mutations for new treatments for rare diseases, and other sub-populations when it comes to cancer. “Drugs are getting licensed based on a relatively small number of patients, so it is incredibly important that pharmacovigilance systems are ready.”
Changing systems
One area that has improved greatly in the past two years is that data on reports of adverse events and side effects held on the Uppsala reporting database is now publicly accessible through a portal, VigiAccess. “It’s been shown that the best way to encourage people to report is to give something back,” explains Chandler, who adds that there is also a move in many organisations – including the FDA and its European counterpart the EMA – to be more transparent.
It took several years to finalise VigiAccess, and it gives the public very basic access to this global database. The first release of VigiAccess has a structure which is recognisable to those who are familiar with the practice of pharmacovigilance,” says Chandler, who adds “hopefully in the future it could be adapted to make it easier for patients to use directly.”
A certain amount of medical knowledge is also required when searching the database. A familiarity with the system used to code adverse events or side effects is also a plus.
Patient groups are already using VigiAccess to help patients with their side effects. Spurrier-Bernard helps people with melanoma search for side effects they are experiencing so that they are better equipped for their next doctor’s visit. “It’s extremely useful, as you can go back to your doctor and tell them to think again about side effects they dismissed, and deal with them. It gives patients extra confidence.”
Reporting apps
New tools are also being rolled out to the public in some countries to help patients report side effects. Apps are being developed on a pilot basis in the UK, the Netherlands and Croatia.
One example is the Yellow Card in the UK, which was a paper-based form and is now available as an app developed by the Medicines and Healthcare Product Regulatory Agency. Its main advantage, according to Chandler, is that “it eliminates the need to track down a paper form.”
While improving reporting is a good start,
Chandler argues that more needs to be done
to help patients manage side effects
Though patients have been able to report in some countries for a number of years, requiring them to find and return paper forms or navigate multiple links online has acted as a significant deterrent, she argues. The development of apps, she says, shows “a lot of progress is being attempted to make it as easy as possible for patients.”
In a similar way to VigiAccess, these apps also offer patients access to data on adverse events and side effects. Spurrier-Bernard was asked for some input about the type of feedback patients would like to receive during the development of the Yellow Card app. “It was really quite cool, as they asked: ‘Would you like data on all the drugs related to melanoma or just your drug?’ It gave people flexibility in what type of feedback they wanted.”
She feels that this feedback is really important, as patients want to know that, if they take the trouble to fill out a report, then something will happen with the data. “Why would people do it if they thought it wasn’t going anywhere?”
Getting the message out
Improving public awareness about the importance of reporting side effects, and how that can be done without going through a doctor or pharmaceutical company, remains a big challenge. One way the Uppsala Monitoring Centre has tried to address this issue is through their ‘Take & Tell’ campaign, which aims to “make pharmacovigilance – monitoring, assessing and understanding adverse effects, or other drug-related problems – into an easily understood, household name… and change the way people view the process of taking medicines and to facilitate dialogue between the health care provider and patient.”
The campaign consisted of posters and other advertising material, such as the ‘Take & Tell’ song, which can still be watched on YouTube, including a reggae version and a version in Chinese.
Some of the countries that participate in their pharmacovigilance programme have limited resources, says Chandler, so the campaign was designed to aid those countries in particular. “It encourages patients to report and is also a general message to everyone to increase awareness that drugs can have adverse events and you can do something about it.”
Patient reporting in the Netherlands
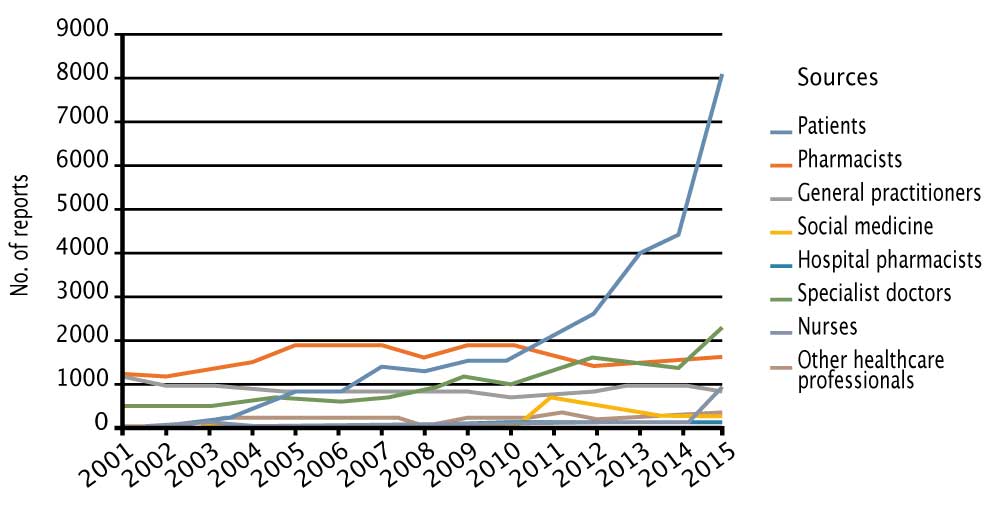
The Netherlands Pharmacovigilance Centre, Lareb, began accepting patient reports in 2003. Fourteen years on, patients are now filing more reports than all other sources put together, with direct reporting having quadrupled over four years (see figure above). Florence van Hunsel, head of signal detection at Lareb, told Cancer World why they initiated patient reporting, and how it has developed.
An initial pilot was completed in 2003. The patient reports submitted during the pilot were analysed, and were found to be very useful. “After the pilot,” says van Hunsel, “we had a culture change in our organisation, as we wanted to be more patient oriented.”
More than 170 patient reports were submitted in the first year, but Lareb wanted to increase that number. They started to advertise the reporting site, and publish their experience. They promoted adverse event reporting in patient magazines, and on patient organisation websites. “One of the most important things is working with patient organisations,” says van Hunsel.
Most recently Lareb produced a series of radio commercials as part of an EU-wide drive to increase patient reporting. The centre also takes part in TV programmes on pharmacovigilance topics. Their efforts led to an impressive increase in patient reports, with more than 8,000 being collected in 2015.
Online forms were always the preferred option for Lareb, says van Hunsel, because it enables them to receive information in a more structured manner, and is more manageable. They recently developed a reporting app, which has been online for a number of months. The hope is that this will further increase reporting levels – 135 reports have already been submitted via the app by patients and healthcare professionals.
As well as direct reporting, Lareb are exploring other ways to improve pharmacovigilance. They are part of the Web-Recognizing Adverse Drug Reactions (WEB-RADR) consortium, which is a large group looking at innovative ways to get pharmacovigilance information. This includes exploring the possibility of data mining of social media, such as Facebook and Twitter, for adverse events, and researching frameworks that need to be in place for this.
Though patient reports are now an important part of pharmacovigilance, van Hunsel stresses that they also need information from healthcare professionals. “I don’t think we would do a great job without them. The mix is ideal.”
Adapting reporting tools
Apps and adverts may improve patient understanding of side effect reporting and make it easier to report them, but tools are also needed to ensure the correct data is recorded on these systems.
Oncologist Perrone feels that more research is needed into the tools used in side effect reporting by physicians and patients. He helped develop the Italian version of PRO-CTCAE, a patient-reported outcome measure developed to evaluate symptomatic toxicity in patients on cancer clinical trials. He suggests that, while it is clear that these sorts of instruments need to be used in clinical trials, maybe they should also be used in clinical practice.
There is a caveat though, as Perrone feels that more research is needed into their use outside of a clinical trial setting. “There is some evidence that patients staying in touch with the clinical team with this kind of instrument may reduce the impact of side effects, and increase quality of life. It may also reduce dependence on the emergency room,” he says.
Side effects reports: flow of information
(click to enlarge)
Individual case safety reports (ICSRs) are submitted to national pharmacovigilance (PV centres), which feed them into VigiBase, the WHO international database at the Uppsala Monitoring Centre (UMC) in Sweden. The data can be searched and analysed using the Uppsala centre’s VigiLyze software, to make it easy for national centres to pull out and analyse relevant data. The Uppsala centre conducts its own analysis, looking for patterns and signals, and reports its findings back to national centres. Since 2015, members of the public have been able to search for side effect reports by drug via the VigiAccess portal.
From reporting to managing – the HIV example
Side effects can be fatal – more often they blight lives. Photosensitivity induced by the B-RAF inhibitor vemurafenib, for instance, turns patients into ‘vempires’, keeping them inside when the sun is out. Poorly controlled diarrhoea keeps people from straying far from a toilet. Sensitive nerve endings can affect mobility and fiddly tasks. Unsightly rashes can also deter people from leaving home. Disturbed sleep patterns can make it hard to function. All of these and more can impact on adherence to potentially life-saving or life-extending drugs. While improving reporting is a good start, Chandler argues that more needs to be done to help patients manage them.
“One area that is currently not being fully addressed in the drug regulatory process, in my opinion, is providing advice to patients and their physicians on how to manage adverse events,” she says. Having met with many patient groups around Europe, cancer patient groups in particular, she feels that as a next step, they need to figure out how to deal with adverse events, so they can advise patients.
Chandler talks about how shocked she was to hear people say that they won’t take their drug that is saving their life, “if they can’t sleep at night, or have a very itchy rash”. Rather than leaving management of side effects with the oncologist or patient, she would like to see regulators having a greater role in providing advice or encouraging research on management of adverse events.
Using her previous role as an infectious disease physician as an example, Chandler says, “the HIV story is remarkable, and they have a lot of adverse events that people have learned to manage.” As people with HIV lived longer and the disease became more treatable, management of side effects became more important. Drugs to treat it can lead to bad rashes, fever, and liver failure, but research into adverse events with HIV medicines uncovered that certain genetic predispositions were found to make people more susceptible. Now patients can be tested to minimise their risk of adverse events.
Many cancers have now reached a similar stage, with prognoses being improved on a regular basis by new innovations. Many people with stage 4 melanoma are now living long enough for side effects to have a real impact, according to Spurrier-Bernard. “Unfortunately, up until three years ago patients with this diagnosis only lived from three to six months, so they had no time to develop a decent reporting system.” New therapies changed that and direct reporting is now vital. “There’s no messing around anymore!”
What does the public get out of it?
People who report side effects contribute to a system designed to improve patient safety, which benefits everybody.
And since 2015, members of the public have also been given direct access to the WHO Uppsala Monitoring Centre database, via VigiAccess, where they can search for adverse event reports on any medication. This can be important in helping make sense of their own experiences and also give them confidence to press the point if their doctor is reluctant to give a fair hearing to their side effects complaints.
Some national pharmacovigilance agencies take on a public information role, publishing the results of their analyses of the side-effect data they receive and providing an information service to respond to specific questions. The Dutch Lareb pharmacovigilance centre, for instance, claims in its 2015 report to have contributed to 10 television and radio broadcasts and 40 articles in the lay press, and responded to almost 2000 queries.
The impact of side effect and adverse event reporting would be all the greater if information gathered on side effects and adverse events was used in a concerted way to improve our ability to manage them.