Cancer patients are put at risk unless the surgeons who operate on them understand the principles of the disease, work closely with other oncology disciplines, and know which patients need to be referred to high-volume specialist centres. This grandround looks at the key surgical factors that influence cancer outcomes, and how to optimise them.
This grandround was first presented by Charles M Balch, MD, FACS, FASCO, Professor of Surgery at the University of Texas MD Anderson Cancer Center, in Houston, Texas, as a live webcast for the European School of Oncology. It was edited by Susan Mayor. Charles Balch is Past-President of the Society of Surgical Oncology and Editor-in-Chief of the Annals of Surgical Oncology. The webcast of this and other e-sessions can be accessed at e-eso.net
Access to surgery is a key issue affecting outcomes in a wide range of conditions, including cancer. The Lancet Commission report on Global Surgery 2030 pointed out that, “Access to surgical care is essential for reduction of mortality and morbidity from surgical conditions” (Lancet 2015, 386:569–624). A subsequent paper on global cancer surgery estimated that 45 million surgical procedures would be needed worldwide by 2030 (Lancet Oncol 2015, 16:1193–224), “Yet, less than 25% of cancer patients worldwide actually get safe, affordable or timely surgery,” warned the authors.
The Commission identified factors associated with poor access to quality cancer surgery, including: lack of investment in public surgical systems; low investment in research and training in surgery; and widespread educational gaps. Recommended solutions included:
better regulated public systems, particularly regarding the training and certification of surgeons,
international partnerships,
super-centralisation of surgical services,
novel surgical clinical trials, and
new approaches to improving quality and scale-up of cancer surgical systems through education and training.
Key Points
A team approach. Almost all cancer patients in the US now receive more than one treatment modality, making contemporary cancer care a team approach combining the collective wisdom of surgeons, medical oncologists, radiation oncologists and pathologists. Managing chronic disease. Developments in effective systemic treatment mean that cancer is becoming a chronic or curable disease, requiring measures to optimise survivorship, manage second primaries, and promote adherence. Continuing education. Oncology is one of the most rapidly advancing specialties in medicine, underlining the importance of validating advances through well-conducted clinical trials and the need for high-quality training and education throughout a surgeon’s career. Specialists and telemedicine. Surgeons who carry out higher voumes of a given procedure achieve better outcomes in patients with complex or advanced cancers, and there is patient and public demand for getting optimal cancer care from specialists and multidisciplinary cancer centres. However, this does not mean that all cancer patients need to be treated by specialists, particularly if they are diagnosed early and their treatment is simple. Innovations such as telemedicine can enable patients to be treated in local hospitals with input from specialists, where required. Supporting standards in general surgery. Surgical oncology specialists should provide educational and research leadership within the general surgery community. Professional societies have a central role in defining the standards for treating surgical patients with cancer and providing education and training to achieve optimal cancer care. Partnerships between societies and medical institutions, including at an international level, will accelerate progress, advance the specialty and improve patient care.
The Commission acknowledged that achieving good outcomes in modern cancer surgery is technically demanding, and noted that outcomes improve when surgery is performed by specialised teams working in high-volume centres, particularly for complex patients and more complicated operations.
Access to high-quality training is essential, with suitable accreditation and quality control for aspiring cancer surgeons. However, this has yet to be achieved by regulatory authorities in many countries. High-income countries, including the US and many in Europe, are driving greater specialisation, but general surgeons also need wider training.
The Commission recommended that surgical professional societies take a lead role in this. It also advised that high- and middle-income countries expand their educational offerings on cancer surgery to low-income countries through bilateral exchanges and greater use of technology-enhanced learning and partnerships, and by including specific curriculum content on cancer in general surgery residency training programmes.
Several organisations, including the US Society of Surgical Oncology, the European Society of Surgical Oncology, the British Association for Cancer Surgery, the European Society for Medical Oncology, the American Society of Clinical Oncology and the (US-based) Health Volunteers Overseas, are all contributing to developing global programmes in cancer surgery.
Why surgeons who treat cancer need to specialise/subspecialise
There have been rapid and substantial advances in cancer research, with new diagnostics and biomarkers, and new systemic therapies including chemotherapy, hormone therapy, targeted therapy and, more recently, immunotherapy. This has led to new combinations and sequences of cancer treatment, including use of neoadjuvant and adjuvant therapies in surgical patients.
There have also been major advances in surgical technologies in the operating room, such as laparoscopic surgery, robotic surgery and intraoperative imaging techniques. The challenge now is to remove cancer with better results, better local-regional control, improved safety and lower incidence of complications. In addition, there is greater recognition of the importance of rehabilitation and restoring function to patients after surgery.
There have also been many changes in the delivery of cancer care, with the development of regional cancer centres and multidisciplinary teams of oncology specialists. This includes surgeons who spend part of their time working as part of a multidisciplinary team, participating in treatment planning with colleagues from medical oncology, radiation oncology, pathology and radiology.
Outcomes for different cancers by risk and hospital type
(Click to enlarge)
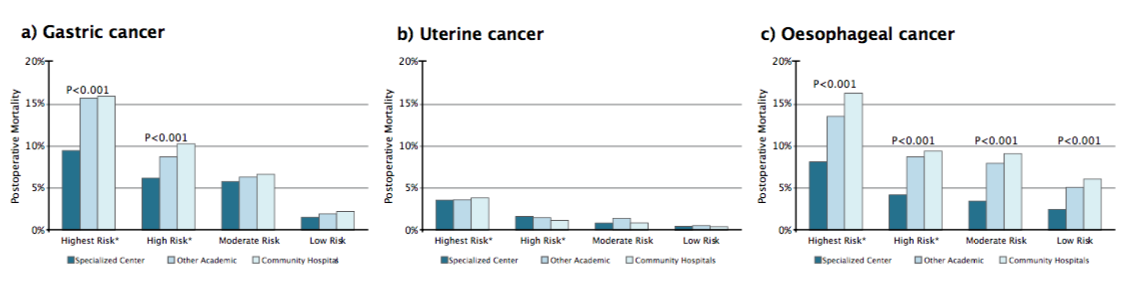
Patients with gastric cancer (fig. a) do better in specialist centres if they are at high risk; patients with uterine cancer (fig. b) do no better in specialist centres regardless of whether they are at high or low risk; all patients with oesophageal cancer (fig. c) do better at specialist centres. Patients with bladder, colon, liver, lung, rectal and renal cancers have a similar pattern of outcomes to those shown in fig. a. Patients with breast, melanoma, ovarian prostate and thyroid cancers have a similar pattern of outcomes to those shown in fig. b. Patients with pancreatic cancer, like those with oesophageal cancer, all do better when treated in specialist centres
Source: K Bilimoria et al. (2010) Ann Surg 251:708–16. Reprinted with permission
Evidence of better outcomes in specialist cancer centres
Well-trained general surgeons can achieve good outcomes in cancer surgery, but it is important they have the judgement as to when complex cases will achieve better outcomes with surgery performed by specialists working in high-volume centres. One example of this was reported in a UK study of breast cancer, which showed that the risk of inadequate treatment of the breast among patients treated by specialists was half that of patients treated in non-specialist units (24% vs 47%, P<0.001), where ‘inadequate treatment’ was defined as treatments where breast-conserving surgery was performed for tumours larger than 30 mm, or if resection margins were positive, or if radiotherapy was omitted (Br J Cancer 2004, 90:1920–5).
The same study showed that treatment by specialists was also associated with a five-fold lower risk of inadequate axillary staging (8% vs 40%, P<0.001) and a nine-times lower risk of inadequate axillary treatment (4% vs 38%, P<0.001). The local recurrence rate, which is a metric of surgical outcome, was 57% lower at eight years (13% vs 23%, P<0.001), and the risk of death from breast cancer was 20% lower for women treated in specialist units, after allowing for case mix and adjuvant therapies. The authors concluded that adequate surgical management in breast centres is fundamental to improving the outcome of patients, irrespective of where it is delivered. This study was conducted in 2004, and since then the UK National Health Service has developed much better cancer centres.
US studies have also shown that surgical volume (i.e. patient case-load) and surgical specialisation both impact, independently, on survival. A breast cancer study showed that surgeons who performed more than 15 breast cancer surgeries per year achieved a five-year survival of 84%, compared with 75% for those who performed 1–5 breast cancer surgeries per year. Risk of death at five years was more than one-third (36%) lower among patients treated by a surgical oncologist compared with a general surgeon, even after controlling for both hospital and surgeon volume, as well as hospital, age, stage, and race (Ann Surg Oncol 2003, 10:606–15).
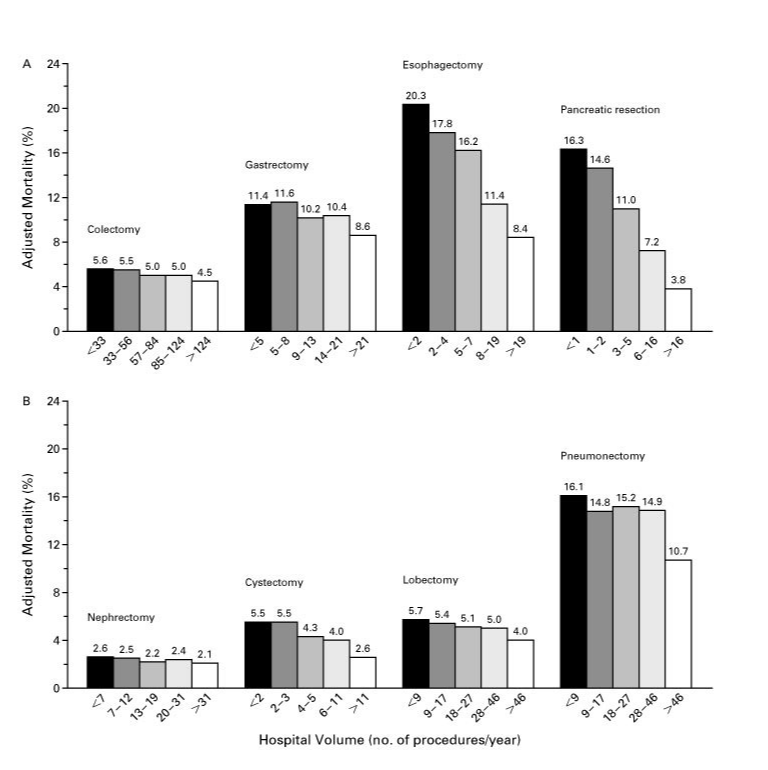
Several US studies have also shown the relationship between hospital volume (the hospital’s annual caseload of patients requiring a particular treatment) and surgical mortality (defined as the rate of death before hospital discharge or within 30 days after the index procedure) varies by type of surgery. Results showed no difference by hospital volume in adjusted mortality for colectomy, which is a more standard operation. However, there was a significant difference by hospital volume in treatment-related mortality after gastrectomy, oesophagectomy or pancreatic resection, (see figure above in Hospital volume and operative mortality).
Another study, this time looking at the surgeons’ annual case-load (NEJM 2003, 349:2117–27), found that for some procedures, including resection for lung cancer or cystectomy, there was little difference in adjusted operative mortality between surgeons with different annual caseload volumes, but for others, including oesophagectomy and pancreas resections, the difference was highly significant (see figure above in Surgeon volume and operative mortality).
A further study showed highly significant differences in 30-day surgery-related mortality in patients undergoing pancreatectomy in relation to both hospital volume and surgeon volume (NEJM 2003, 349:2117–27). Mortality was 18% in hospitals managing fewer than one case per year, compared to 4% in hospitals with more than 16 cases each year. Mortality was three times lower in patients treated by surgeons with more than four cases a year compared to those with one case per year (5% vs 15%).
Patient risk factors
Stage at presentation and comorbidity, particularly in older people, are more important influencers of cancer outcomes than the annual number of similar patients treated by their surgeon or at their hospital.
Studies comparing postoperative mortality in specialised centres with other academic centres and community hospitals in the US have shown that treatment at specialist centres is particularly important for ‘high-risk’ patients with some cancer types, but not others (see figure above in Outcomes for different cancers by risk and hospital type).
High-risk patients with bladder, colon, gastric, liver, lung, rectal and renal cancers had improved outcomes when surgery was performed at specialised centres compared to community hospitals, but there were no differences for moderate- or low-risk patients (above left). However, no such difference in outcomes was seen for high-risk patients with breast, melanoma, ovarian, prostate, thyroid and uterine cancers (above centre).
For patients with cancer of the pancreas or oesophagus, treatment at specialist centres was associated with lower postoperative mortality compared to other hospitals, regardless of the patient’s level of risk (above right).
Training of oncologic surgeons and general surgeons in cancer surgery
The US Society of Surgical Oncology and the European Society of Surgical Oncology recently published two important papers on the training and education of cancer surgeons. The first showed very large variations in the training of surgical oncologists around the world (Ann Surg Oncol 2016, 23:1769–81). The second proposed a global curriculum in surgical oncology that can be used both for training general surgeons and also as curriculum recommendations for training surgical oncology specialists, who are very important at the national level for managing complex patients and for leading training programmes for general surgeons (Ann Surg Oncol 2016, 23:1782–95).
Both the US and the global curriculae defined the distinguishing features of a surgical oncologist as an excellent surgeon who:
can safely manage cancer patients through complex operations, and has the judgement to know which operations to select
knows how to integrate surgical treatment as part of a multidisciplinary team, including the type and timing of surgery after pre-operative systemic therapies and/or radiation therapies
participates as an oncologist in long-term disease management of cancer patients.
How preoperative treatments are changing the role of cancer surgery
An important part of the surgical management of patients who present with stage 3 disease is the increasing preoperative use of medical therapies including chemotherapy, targeted therapies and immunotherapies. This is going to change how we manage patients surgically. For the majority of US patients with stage 2–3 breast cancer, and in many centres in Europe, systemic therapy is now the first treatment, and surgery the second. This requires a lot of planning with medical oncology colleagues around the timing of surgery and the role of the sentinel node, which is different in this setting. This approach represents the future of treatment for many cancers, for which breast cancer is the prototype.
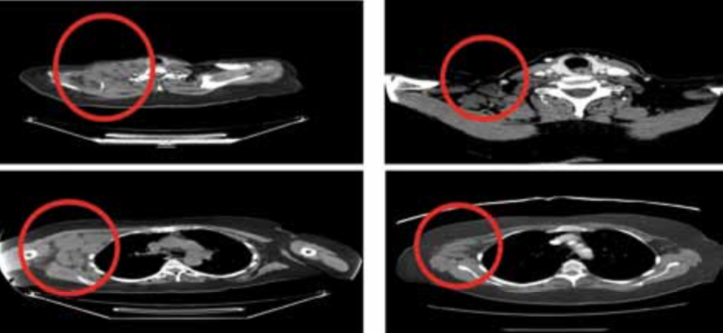
The figure above shows an example of a patient with a bulky and unresectable advanced melanoma in the groin and pelvis, treated with anti-PD1 immunotherapy. Tumour shrinkage after immunotherapy facilitated surgery. The patient had a pathological complete response, which could not have been staged without surgical resection of the tumour masses that were originally detected.
The increasing number of effective systemic therapies will impact on the management of surgical patients. Many of these are administered orally, and many are less toxic than traditional chemotherapies. Examples of new oral and subcutaneous agents that are available for a variety of cancer types include: anastrozole, capecitabine, gefitinib and sunitinib. More than 1,000 new cancer drugs are in various stages of clinical development. Some dramatic examples of tumour shrinkage have been seen with agents such as the targeted BRAF inhibitor vemurafenib in metastatic melanoma with V600E mutation. Another major advance is the development of immunotherapy such as immune checkpoint inhibitors, which have now been shown to be active in more than 17 different types of cancer. These agents will be used increasingly in surgical patients, and the sometimes dramatic treatment responses achieved in patients with advanced disease indicate that they will translate into benefits in patients with earlier disease.
An example illustrating the future of how these new therapies impact on cancer surgery is shown in the figure overleaf, which shows the response of a very large melanoma metastasis after a single dose of combination immunotherapy. The patient had a pathological complete response demonstrated by surgical excision of the remaining tissue (NEJM 2015, 372:2073–4). A more famous example, former US president Jimmy Carter, has been in complete remission for more than 14 months [as of July 2017] after treatment with a single dose of an anti-PD1 checkpoint inhibitor, following presentation with liver and brain metastases from metastatic melanoma at the age of 92.
Preoperative immunotherapy in advanced melanoma
Increasing use of preoperative systemic treatments is changing the role of cancer surgery, requiring ever closer team work between disciplines
Source: Images courtesy of Dr Merrick Ross, University of Texas, MD Anderson Cancer Center
Response of melanoma to immunotherapy
A single dose of ipilimumab plus nivolumab resulted in complete pathological response of this large metastasis in the chest wall of a patient with melanoma
Continuing education for practising surgeons is essential. There are a variety of ways that this can be provided, including live meetings such as those run by the US, European and British surgical oncology societies, SSO, ESSO and BASO, and also through affiliations with tertiary centres, such as the one between community hospitals and the MD Anderson Cancer Center. There are also continuing medical education (CME) initiatives led by journals such as the Annals of Surgical Oncology and the European Journal of Surgical Oncology, both online and in print versions, and training initiatives conducted by live webinars such as those provided by the European School of Oncology. The US Society of Surgical Oncology now runs a compulsory self-assessment programme, to help surgeons keep up with the field.
Telemedicine is increasingly being used both for medical education, especially for physicians in community settings and rural areas, and for specialist consultative services, particularly in supporting shared decision making about individual patients between doctors working in different locations and even in different countries.
Telemedicine is increasingly being integrated into the operations of US hospitals, speciality departments, home health agencies, private physicians’ offices and, in some cases, even for educational purposes in the patient’s home or workplace. The technology enables the sharing of X-ray, pathology and even ultrasound images, in real time and in high resolution, between locations.
Telemedicine specialist consultations and virtual tumour boards can bring together specialists from different countries to discuss complex cancer cases anywhere in the world. A study reported at ASCO 2016 showed that 91% of participants in virtual tumour boards found it very helpful in managing their patients; 100% felt quality of patient care was improved; and 100% considered their own confidence improved (JCO 2016, 34:211).
International relationships with individuals and organisations can be of assistance in consultations, reviewing complex patients, and in the education of surgeons in local communities and nationally.
Impact of quality improvement programmes on surgical quality
The National Surgical Quality Improvement Program (NSQIP), run by the American College of Surgeons, now operates in most US hospitals (Ann Surg 2009, 250:363–76). An evaluation of the impact of NSQIP demonstrated what a difference this type of programme can make at a national level.
Results showed that two out of three hospitals (66%), including community hospitals, reported lower mortality rates, and more than four out of five (82%) reported lower morbidity rates.
The poorest-performing hospitals, with low volumes at surgeon or hospital level, were more likely to improve, but even high performers improved. The number of low outliers (with low mortality/morbidity) increased, and the number of high outliers (with high mortality/morbidity) decreased, which is very encouraging for a programme initiated nationally. It was estimated that the programme was associated with each hospital avoiding an average of 250 complications per year.
Advocating for quality cancer surgery
Professional bodies, together with governments in each country, need to insist that their citizens receive high-quality care. This includes ensuring there are well-trained surgeons, that cancer care is well organised nationally, for instance with regional specialist cancer centres, and that relationships are developed internationally with individuals and organisations that can be of assistance.
Surgeons working in communities should facilitate sharing of knowledge, and support young surgeons working in cancer, encouraging them to engage with leading specialists and networks in the field. Governments should raise expectations for high-quality and timely care, working within their resources to achieve that over time.




This grandround was first presented by Charles M Balch, MD, FACS, FASCO, Professor of Surgery at the University of Texas MD Anderson Cancer Center, in Houston, Texas, as a live webcast for the European School of Oncology. It was edited by Susan Mayor. Charles Balch is Past-President of the Society of Surgical Oncology and Editor-in-Chief of the Annals of Surgical Oncology. The webcast of this and other e-sessions can be accessed at e-eso.net

A single dose of ipilimumab plus nivolumab resulted in complete pathological response of this large metastasis in the chest wall of a patient with melanoma