While many western countries are pioneering safe delivery of more cancer care in primary, community and home settings, across central and eastern Europe, beds in university hospitals and cancer centres are still filled unnecessarily with people requiring diagnostic procedures, routine care and check-ups. Marc Beishon looks at the implications and explores prospects for change.
When healthcare analysts examine disparities in outcomes among cancer patients in Europe they often focus on availability of treatments such as new oncology drugs and access to radiotherapy, and on screening, late diagnosis and prevalence of risk factors, especially smoking. Underpinning the discussion is expenditure on healthcare, and there is a stark divide between central and eastern Europe (CEE) countries and those in western Europe in what is spent on health. Luxembourg and Norway, at one extreme, spend almost seven times more per person than Albania and Romania, at the other.
The relationship between health spend and cancer outcomes is by no means straightforward, however – a point that was acknowledged by a group of clinicians from CEE countries in 2016 paper which set out recommendations on the changes needed most to pull up standards of oncology care in the region (Oncologist 2016, 21:1183–90).
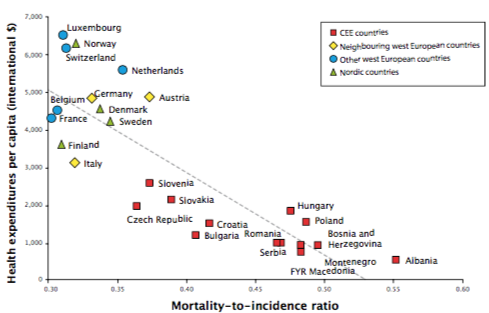
Certainly, they say, even allowing for lower costs of some inputs, with such large disparities in healthcare budgets it is not realistic to expect outcomes comparable with western countries. Yet plotting per capita health expenditure against outcomes (measured as the mortality-to-incidence ratio) shows that some countries get much better results than others for an equivalent health spend, which indicates that some countries could be spending their money a lot more effectively.
While Austria spends more per capita on health than Sweden, note the authors, Sweden has had a significantly better mortality-to-incidence ratio for all cancer types. A similar equation holds for Switzerland, which spends per capita 72% more on health than Finland, for an equally good mortality-to-incidence ratio. Within the CEE region, looking specifically at spending on oncology drugs, the authors point out that the Czech Republic achieves a significantly better mortality-to-incidence ratio in breast, lung, colorectal, and renal cancers than countries like Hungary, Croatia and Poland, which spend a similar amount.
Achieving the best benefit from health spending is becoming increasingly pressing, as the rising age profile and high costs of sophisticated new health technologies push health budgets to their limits. A major focus, not least in cancer, has been to limit the involvement of expensive in-patient care to where it is really needed, and transfer a lot of care delivery to outpatient, primary and community services.
When done safely and well, this can benefit patients, who are more able to get on with their own lives. And while developing the capacity of other services to play this role requires serious investment, taking the burden off high-end tertiary services should result in overall savings.
Effecting such system-wide changes is never easy, but many health services have been trialling these principles in various cancer care settings for many years now. The trouble is, the great majority of that work is being done in western countries, whereas it is the health services of CEE countries – the ones with the smallest per capita health budgets – where the reliance on hospital-based care is greatest.
This is a point that was flagged up by the authors of the Oncologist article, who in their recommendations call for the current preference for in-patient/hospital-based care in CEE to be changed to modern forms of ambulatory, day hospital and clinic treatments, “as day and ambulatory treatments may be superior in both direct and indirect costs, as well as quality of life for patients and families”. They also call for the development of clinical guidelines and training for general practitioners (GPs) for management and follow-up of cancer patients and survivors.
Excessive in-patient use
The extent of overuse of in-patient care across CEE countries may surprise some who are unfamiliar with the region. In most hospitals that treat cancer in western Europe, outpatient care for routine treatments such as intravenous chemotherapy and radiotherapy are the norm. Instead, in CEE countries people are often admitted to hospitals as in-patients to receive the same treatment, taking up expensive beds and hospital resources that could be better used to improve care. It is a hangover from the centralised Soviet-style healthcare that has been neglected for reform, mainly by authorities in charge of health policy.
“Hospitals have inherited a centralised structure and continue to apply a model that isn’t applicable to modern cancer treatment”
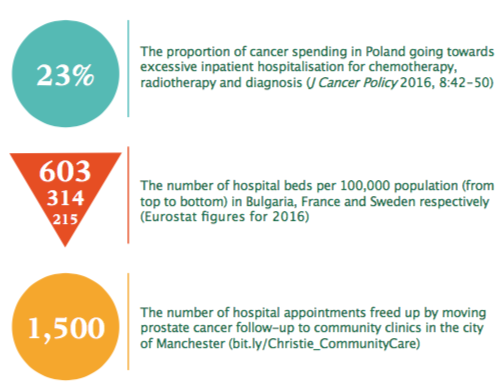
Paradoxically, this means that some CEE countries have more in-patient beds per 100,000 people than most in western Europe, which some might see as a positive indicator – but which in most cases indicates a potentially wasteful use of resources. For example, figures for 2016 from Eurostat show that Bulgaria had 603 beds per 100,000 population, while France had only 314, and Sweden had among the lowest, at 215. Lithuania, Romania, Poland and Hungary also had high bed numbers, as did some western European countries – a possible indicator of the way their healthcare systems are managed: Germany, at 606 tops the list, and Austria and Belgium are also high up the order. Comparisons are not definitive, as some countries count psychiatric beds in their ‘curative’ bed count, and Germany’s count is higher still if its tradition of providing rehabilitation in-patient beds is included.
As Alexandru Eniu, a medical oncologist at the Ion Chiricuta cancer institute in Cluj-Napoca, Romania, and co-author of the CEE paper, comments, today’s hospitals in CEE countries have inherited a centralised structure and continue to use a disease model that just isn’t applicable to the multiple visits that modern cancer treatment requires. It is mainly the reimbursement systems that continue to support this out-of-date model, he adds. While having centralised systems is good for consolidating expertise, there are fewer centres and it means that patients often have to travel long distances to receive treatment, and they do not receive financial help with transport or with staying in hotels near to hospitals. “And in Romania, as with other CEE countries, a key obstacle has been that state reimbursement in public hospitals is mainly for in-patient care, with little allocated for outpatient departments – and this is still the case.”
“Reimbursement in public hospitals is mainly for in-patient care”
This means that procedures which in western Europe are routinely done on an outpatient basis, such as chemotherapy, CT scans and radiotherapy, are often carried out on patients admitted to hospital over several days, simply because hospitals are reimbursed at a far greater rate.
As Eniu, who is a breast oncologist, says: “If I have a patient receiving a cycle of adjuvant chemotherapy there is no need to hospitalise her – but if I do it in our outpatient department the hospital gets paid a great deal less than if she is admitted as an in-patient say over three days. This is a bad incentive and the difference in income is big.”
Cancer outcomes by per capita health spend
Mapping per capita health spend against cancer outcomes, measured by the ratio of deaths to new cases (all female cancers), shows that health spend has a big impact on outcomes, but some countries spend their health budgets much more e ectively than others Source: E Vrdoljak et al (2016) The Oncologist 21:1183–90, republished with permission
For radiotherapy, there are different pressures at work. While hospitals are not financially incentivised to admit patients for the full five or six weeks often needed for a course of therapy, the shortage of machines in the region mean patients often have to travel long distances to receive treatment. If they cannot afford accommodation, they could miss out on care unless hospitals admit them for the full period.
The upshot, says Eniu, is that care is compromised in several ways. Admitting patients for long periods means delays for other patients who must wait for a place; people may forego treatments as they cannot afford the time or money to receive inflexible, in-patient care; and the inefficient use of resources means that there is shortage of funds for the treatments themselves. Eniu says that in Romania there is still concern about access to essential drugs, let alone new targeted agents. “If you don’t have cisplatin for lung and testicular cancer it’s hard to worry about a lack of TKIs,” he says. “If you hospitalise people for CT scans you don’t have money to spend on other things.”
There are outpatient facilities though – at Eniu’s hospital a majority of chemotherapy is delivered there but only through staff working probably double time in overcrowded conditions with little regularised income to fund the department. It is a juggling act between in- and outpatient resources, and it is not possible to hire more people, he adds. “We also have little time for other services such as patient education and management of side effects – we can only focus on essential treatment. Our treatments are good, but quality in cancer care means integration and paying attention to detail. We know that our patient experience is not the best; our care in alleviating fears and symptoms is lacking compared with western Europe.”
In Romania, Eniu places much of the blame on a lack of a national cancer plan – it is hard to attract more money for cancer, or make more of existing money, as it is addressed just as other diseases, and hospitals are funded with the general disease-related-group system for reimbursement. “This is suited to episodes of treatment and not for cancer, where you may not see outcomes for many months and patients need to come in for different things at various times.”
Healthcare culture
It’s a point echoed by Richard Sullivan, director of the Institute of Cancer Policy at King’s College London, who says that everything stems from the overarching health policy in countries – “How is health seen generally? and how is cancer seen?” The big picture tends to set the agenda, and smaller challenges further downstream often won’t be tackled well if cancer is still seen by policymakers as just a serious hospitalised condition.
That said, it is not just politicians and policymakers who set the agenda, although state insurance systems that incentivise in-patient care are a major component of lack of resources. Sullivan says that entrenched healthcare culture – such as always admitting people for radiotherapy – plays a part, and indeed is manifest in other countries such as Germany, as well as being a hangover from Soviet times. The ‘ego’ of clinicians who insist on seeing patients in the acute setting can also be a factor, he says, and can be reinforced by ‘dyadic’ relationships with patients who express preferences to always see them.
“Entrenched healthcare culture, such as always admitting people for radiotherapy, plays a part, as does the ego of clinicians”
Paying for favours from doctors is also still part of the culture in many CEE countries, and it has been reported by Transparency International that in Lithuania one in four people who visited a healthcare institution admitted to paying a bribe. Patients also face co-payments for their care, and they generally lack trust in, and receive little support from, their general practitioners to help them navigate their cancer journey.
Sullivan cautions, however, that outpatient settings are not necessarily panaceas for cost savings and efficiency, because of the growing number of toxic treatments and complex surgical interventions. The emphasis must, he says, be on high-quality multidisciplinary treatment in high-volume centres that embraces concepts such as enhanced recovery after surgery (ERAS) to minimise readmissions. It must also be recognised that outpatient settings will need more resources for a wide range of treatment and survivorship care, often for older people with complex needs. He also stresses that palliative care is increasingly important in cancer and is adding to pressure on in- and outpatient costs.
Sullivan is a firm believer in collecting data that can inform policy rather than relying on modelling to improve quality. He mentions Avedis Donabedian’s landmark work on health quality frameworks: “This won’t tell you what is wrong but identifies outliers,” he says.
Poland in focus
Poland looks to have followed this advice in analysing activity and spending as a precursor to recent cancer care reform.
A 2016 paper led by Barbara Więckowska at the Warsaw School of Economics found that spending on cancer in 2012 accounted for 6% of healthcare and more than 10% of the services funded by the country’s National Health Fund (J Cancer Policy 2016, 8:42–50). A mere 8% of the spend was on ambulatory care, and only 39% was on day case admissions. The authors reported that excessive hospitalisation in chemotherapy, radiotherapy and for diagnosis accounted for 23% of total cancer spending, and that Poland had more in-patient bed days than England (5.3 million vs 3.2 million), even though it had half the reported number of new cases.
Given that the share of health spending on cancer was about the same as for other countries, the authors commented that there was “a huge window of opportunity to restructure the financing mechanism for oncology in Poland”. They found that 50% of all admissions and 28% of money were spent on purely medical admissions and small diagnostic procedures such as a CT scan and bronchoscopy – involving no surgery, chemotherapy, radiotherapy or any other active treatment. Together these cost about five times more than had they been delivered in the ambulatory setting. Making savings would release funds for rapid diagnosis, surgery and ambulatory radiotherapy, and providing hostels and transport for patients where daily travel is currently not feasible.
A recent paper looked at how effective changes have been in Poland’s cancer reform, noting progress in introducing waiting time limits, multidisciplinary consultations, and a care coordinator position (Int J Health Plann Manage 2018, doi:10.1002/hpm.2635). But there is still a long way to go in centralising specialist treatment and addressing fragmentation, and shifting diagnostics and treatment to outpatient settings – moves that have been “recommended by numerous Polish national experts as contributing to both the cost-containment objectives and improvement in health outcomes”.
Moving away from in-patient care
There are numerous initiatives, especially in western Europe, that aim to provide better patient-centred cancer care in the outpatient setting. For example, a number of locations in England have established nurse-led clinics in primary care practices to care for prostate cancer patients; Ireland has an oncology education programme for community nurses that was set up in response to the country’s national cancer strategy; Sweden has a number of cancer rehabilitation centres staffed by multidisciplinary teams. In Liverpool, England, women can even receive a certain drug treatment in their own workplace, thanks to a version of trastuzumab that can be delivered by nurses subcutaneously, and several health districts have mobile chemotherapy units in large trucks.
There is also growing interest in using routine remote symptom monitoring to ensure timely help and advice for people undergoing chemotherapy, while avoiding unnecessary hospital check-ups. One example is the Advanced Symptom Management System (ASyMS) remote technology currently being trialled across Europe for people undergoing chemotherapy for breast, colorectal or haematological cancers (see BMJ Open 2017, 7:e015016).
Even people being treated for diseases like acute myeloid leukaemia, where the treatment makes them highly vulnerable to infection, are being offered the option of spending their treatment period at home, and in the case of one Danish haematology department, even get to self-administer their own chemotherapy (see picture below).
Mobile chemotherapy units like this one, which was provided by a charity working with the UK’s National Health Service, enable patients to safely receive treatment close to home (www.hopefortomorrow.org.uk)
The new systems for delivering care still cost in staff time and resources, especially if other clinic facilities have to be set up. A community prostate cancer initiative started by the Christie cancer centre in Manchester, England, for instance, reported that more than 1,000 patients have been moved into community follow-up clinics set up in six locations, with more planned. On the plus side, this freed up more than 1,500 hospital appointments. A majority of men were able to self-manage when supported with the right advice, so cost savings are likely as well as less tangible benefits in quality of life.
Pushing the boundaries of home-based care
An outpatient chemotherapy service that not only keeps patients out of hospital but even allows them to manage their therapy at home has been developed at Denmark’s Rigshospitalet by Lars Kjeldsen, head of the haematology department. As he explains, there is considerable pressure on hospital resources, as medical expenses keep on rising, and one way to spend more on say new drugs is to save on inpatient beds and related staff costs.
Patients who often take up lot of bed time are those treated for acute myeloid leukaemia (AML), as it has an intensive complex chemotherapy regime that can induce bone marrow failure and low white blood cell counts, which increases risk of infection. “We were admitting patients for as long as three to four weeks following chemotherapy if their counts were low, to prevent infection,” says Kjeldsen.
That started to change more than 10 years ago when patients were first given prophylactic antibiotics and sent home to monitor themselves, but what was missing was also delivering the chemotherapy, which often has to be scheduled for as long as 30 days during treatment periods. Now certain patients, especially those with support at home, can take home several doses of chemotherapy that are delivered by a programmable digital pump into a central line, and they just return for refills.
This change of management for AML patients, and other initiatives such as pump-administered antibiotics, has allowed Kjeldsen to close 10 beds in his haematological department, cutting the number to 42 from 52, but he says there have been obstacles. There has been little support from doctors as they are, he says, mainly interested in prescribing drugs, not in how they are delivered. It needed financial support to get off the ground – in this case he had to rely on an innovation award. “We need to spend more money to change things in healthcare,” he says. Then there is evidence that it would work: “Some said we should do a randomised trial, but sometimes you set out to prove things that are self-evident and an RCT would only have served half of the patients. Instead we made the change and gathered information to prove it was feasible and safe, and we have had few patients coming in with severe infections or problems with the pump.”
Patients are always in touch over the phone if they have problems, he adds, but to expand services like this, primary healthcare professionals also need to take on certain aspects such as supervising intravenous antibiotics, as hospital resources will always be limited. Kjeldsen also notes that as more people get more treatments given the introduction of new drugs and regimes there will also be a growing number of very sick patients who cannot be taken care of at home and they will require inpatient care from existing staff.
A 2018 paper by Kjeldsen and colleagues details the use of home chemotherapy administration for AML and lymphoma patients (see Br J Haematol 2018, 181:637‒41)
Primary and community care
This also indicates that it is not just in-patient but also outpatient resources in hospitals that could be freed up, and a direction of travel is now back towards primary care, which is the gatekeeper to cancer services in countries such as the UK. This is not just GPs, but also community pharmacists, psychologists, nurses, occupational therapists, geriatricians and others, including the army of unpaid carers (informal care costs for breast cancer alone in Europe are estimated at more than €3 billion a year – more than 20% of the entire care costs, according to research by Sullivan and colleagues – Lancet Oncol 2013, 14:116–74).
Making savings would release funds for rapid diagnosis, surgery and ambulatory radiotherapy
Primary care is likely to come under increasing pressure to be involved in the care pathways of cancer patients, especially in optimising physical and psychosocial care during extended periods of treatment and survivorship. Social care, especially for older patients, is also vital. A Lancet Oncology Commission of 2015 examined in great detail the expanding role of primary care in cancer control, noting that shared care approaches between primary care and oncologists is key, with evidence from the US that patients who see both are most likely to get the full array of care they need.
Developing the role of primary care, particularly the pivotal role of the GP, in follow-up and survivorship care of cancer patients faces significant barriers, in time, education and communications with specialists. While GP practices in countries such as the UK have expanded to be multiprofessional and based in much larger facilities, if GPs are to take more responsibility in cancer their role needs to be formalised, with guidelines for the many subgroups of patients, as Annette Berendsen commented in Cancer World in 2018 (‘In the Hot Seat’, issue 82).
In the CEE region, Eniu comments that primary care involvement in cancer is rudimentary and GPs are fearful, and few think they can help, further burdening already overcrowded hospitals. Indeed, Sullivan also comments that in some countries patients are simply lost to primary care altogether and are destined to seek care only at secondary level.
In-patient care across Europe: the numbers
The sequence of European cancer initiatives – EPAAC (European Partnership for Action Against Cancer), CanCon (the Cancer Control Joint Action, which published the European Guide on Quality Improvement in Comprehensive Cancer Control) and now iPAAC (Innovative Partnership for Action Against Cancer) have all addressed the governance of integrated cancer care and national policy in various ways, as have a number of European cancer societies. But the structure of national healthcare systems and changes in political direction can be frustrating barriers to progress (see also Spotlight on moving towards an integrated cancer care network in the Czech Republic).
In the UK, the government has published an ambitious 10-year plan for the National Health Service that promises to boost out-of-hospital care, and “finally dissolve the historic divide between primary and community health services”, and increase the use of digital technologies such as video consultations. A key aim is to reform outpatient services to reverse a major rise in visits. Cancer patients should have access to a personalised care plan and rapid access to clinical support.
The capacity of a health system to embrace holistic and community-focused cancer care alongside all the other competing chronic conditions will be a big test, but one that people will value, considers Sullivan. “People want to be normal and not be never-ending cancer patients. Disease is not a normal state of being.”