What does an ideal cancer service look like and how can countries/regions make that transformation? A European collaborative project spent two years trying to answer this question. The solution they came up with is now being piloted in the Czech Republic, as Sophie Fessl reports.
“How do you reconcile providing cancer services near a patient’s home with ensuring they get the best possible care?” It’s the fundamental question that has been asked in every country and region where efforts have been made to reorganise fragmented cancer services into a coherent structure able to optimise the experience and outcomes of every patient.
Sweden, England, the Netherlands, France, Ireland, Portugal, Italy and Spain, are some of the countries that have gone a long way towards developing and implementing their own solutions, each applying a broadly similar set of principles, adapted to the culture and structure of their own health services.
Yet in the majority of countries, particularly in central and eastern Europe, efforts to improve the way cancer services are delivered have hardly begun. As a result, big improvements in standards of diagnosis and care over recent decades have often been limited to flagship national cancer centres, while the majority of patients are still being diagnosed and treated in facilities that lack the necessary mix of expertise, teamwork, and governance. This failure to raise standards across entire systems is hampering efforts to close the east–west survival gap.
Even among countries that have done a lot to ensure that treatments are planned and delivered by the right people in the right places, diagnostic, primary and community care services often remain poorly integrated, hampering access to early and accurate diagnosis, and psychosocial, supportive and survivorship care.
Finding ways to guide and to galvanise countries to improve the integration of cancer services has been one of the more ambitious projects of the European Joint Actions on cancer – a series of three-year voluntary collaborations between EU states aiming to improve national capacity and European coordination in cancer control and care (see also In the Hot Seat).
“I was never hoping for as much: that, within the life span of the project, we would have a CCCN built ex novo, based on the CanCon principles”
As part of the CanCon Joint Action (2014–17), Lucio Luzzatto, a former director of the Tuscan Cancer Institute, in Italy, led a project on ‘comprehensive cancer care networks’, which sought to define the key elements of a networking model that could be implemented in any territory, to enable people to access the best and most comprehensive pathways for cancer care as near as possible to where they live, “through the synergy of all relevant institutions that have complementary expertise,” (CanCon Executive Summary 2017).
The concept was broadly based on an approach developed and implemented across the Tuscan region, drawing also on the experience and expertise of collaborating partners from many European states including France, Germany, Ireland and Norway. But it was the involvement of the Czech Republic, which had less experience in restructuring cancer services than any of those countries, that arguably did most to ensure this project will have real relevance and impact in the countries that need it most.
The Czech participants, led by Ladislav Dušek, from the Masaryk University Institute of Biostatistics and Analyses, were so convinced by the idea that they decided not only to talk the talk but also walk the walk, by implementing such a comprehensive cancer care network as a ‘real-life, real-time example’.
The concept developed through a European collaboration is now being taken through a test drive in Vysočina and Southern Moravia, neighbouring southern regions which are considered broadly representative of the Czech Republic as a whole. With a combined population of 1.7 million inhabitants, they are large enough to be self-sufficient in all cancer diagnoses, including childhood cancer, according to Dušek.
“We were very lucky that in the Czech Republic they became very enthusiastic about this idea,” says Luzzatto. “Ladislav Dušek, in particular, said ‘why don’t we do this’? I was never hoping for as much: that within the life span of the project, we would have a comprehensive cancer care network built ex novo, based on the principles defined in CanCon. But that is what happened.”
The hope is that the Czech example will offer a real impetus to other countries and regions that may be struggling to build the momentum and political will to restructure their own cancer services.
Speaking at the Regional Cancer Control Baltic Policy Conference held in Riga in January 2017, Dušek explained why he had found the network idea to be so attractive within the Czech setting. “By 2013, regional cancer centres were established in all regions. But we still faced a growing inequality in cancer care, and cancer centres even started competing with the general hospitals in their catchment area… At this time, the key words of cancer care were ‘inequality’ and ‘competition’. The main question was: how do we manage the growing burden of prevalence, and how patients should be treated? I really appreciated the idea of networking. … Networking is communication, it is the organisation of community-based services for all patients in the catchment area.”
Defining the ideal network
The basic idea behind a comprehensive cancer care network, explains Luzzatto, is to provide access to all the different elements of cancer care that are covered by leading comprehensive cancer centres – from diagnostics to care planning, treatment delivery, supportive care, psychosocial support, palliative and survivorship care, and research – but without having to have everything focused in a single centre.
This was the concept he and colleagues at the Tuscan Cancer Institute developed and set up in 2003 to raise standards of care across the region. “Without moving either patients or cancer care experts, we built a strong network of as good a quality as a major centre, but diffuse. This is how we came up with the term comprehensive cancer care network – or CCCN for short.”
“Comprehensive cancer centres are certainly a good thing,” he says. “The long established ones, like the Royal Marsden, Memorial Sloan Kettering or Gustave Roussy, are unquestionably good, and a part of history. However, the reality even in Europe is that cancer is not always treated optimally. When someone in a small town is treated locally, I’m not sure if the care is always up to the standards of major institutes. The notion of a CCCN is to form a network that is as good as a comprehensive cancer centre, but multi-centric. It is as simple as that.”
While the concept may be simple, getting a network to work rarely is. Luzzatto says he and his CanCon collaborators spent nearly two years defining the key elements of a comprehensive cancer care network. “We worked very hard because we wanted to distil the essentials.”
“The notion of a CCCN is to form a network that isasgoodasa comprehensive cancer centre, but multicentric. It’s as simple as that”
CCCNs, as defined by CanCon, are made up of units and institutions along the pathway from research, prevention and diagnosis to end-of-life care or survivorship. They are characterised by:
a formal agreement for cooperation among network partners,
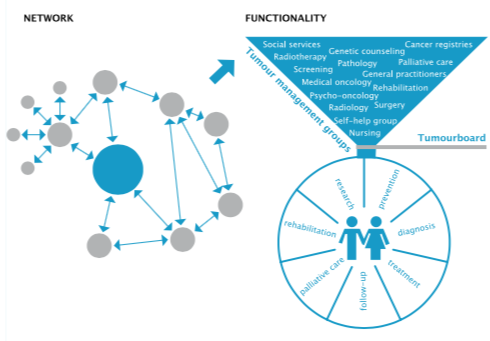
interprofessional teams that work together in tumour management groups,
treatment protocols that are the same across all hospitals in the network,
a quality assurance system, and
a common IT infrastructure.
Together, these measures aim to improve quality of treatment and outcomes for all people living in an area. Patients, expertise and data are all supposed to flow between the participating institutions. Multidisciplinary, tumour-specific tumour management groups provide care to all patients with a specific tumour living in the CCCN’s catchment area.
Luzzatto sees some of the elements as non-negotiable, but others less so, which he says can be an advantage. “The beauty of the CCCN concept is that it is flexible. The networks set up in different places need not be identical, as we do not intend to impose a hard and fast template. At the Istituto Toscano Tumori, which certainly served as a model, we have three major centres in Florence, Pisa and Siena that work together in the network, alongside other units throughout the region of Tuscany. The CCCN in the Czech Republic is rather different, as one major institute already existing in Brno [South Moravia] was clearly the hub around which a network could be built. So there, the network is essentially a centre with several satellites.”
CCCN essentials ‒ the CanCon recommendations
Equal access
To reduce travel distance to quality cancer care, access points and patient pathways within a comprehensive cancer care network (CCCN) should be clearly defined, with access points as close as possible to where patients reside, and uniformly optimal care should be provided as close to home as possible.
Structure and governance
CCCNs should be multicentric, combining units dealing with the management of all aspects of cancer care. These units will be in different locations and under a single governance structure. They should collaborate consistently in a structured way, to pursue their common goal with greater effectiveness and efficiency.
High-quality care
CCCNs should adopt a multidisciplinary personalised approach based on tumour management groups integrating specialised hospital care with care in the community, palliative care, psychosocial support, rehabilitation and survivorship care. Quality of care should be measured with quality indicators. A process for continuous quality improvement should be put in place and implemented. For each type of rare cancer, a unit within the network should be identified that can provide the necessary expertise. If for a certain cancer no suitable unit can be identified, patients should be referred to an appropriate unit outside the CCCN.
Research
CCCNs should take full advantage of the proximity of patients, researchers and care providers to pursue high-value basic, translational, clinical outcome and population research programmes to support the delivery of optimal patient care within the CCCN.
Setting up a CCCN: when and how
Given the benefits that a CCCN can provide with respect to equity of access as well as quality of cancer care, it is recommended that the creation of one or more CCCNs be always considered when making decisions about the structures and governance of cancer care. Where an area is already served by a comprehensive cancer centre, a CCCN can be built around it. Performance indicators and evaluation models should be defined from the outset of the network.
The full CanCon summary of recommendations for comprehensive cancer care networks can be found at CancerControl.eu
Piloting the concept in real time
Addressing an audience of Baltic-region decision makers, at the Riga Cancer Control Conference, Dušek described how they went about organising their fragmented cancer services into a CCCN “as a cascade of many steps”. The first step was to change the data protection laws to allow the centralised sharing of data between hospitals and registries that is required to “predict capacities, budget impact, and numbers of patients to be treated”.
These data were then used to get local and national political support for the idea of establishing a CCCN. Finally, the reimbursement system had to be changed so that the CCCN could be accepted by health insurance companies – the payers in the Czech healthcare system.
Common governance is achieved through managerial leadership that coordinates the network, a clinical leadership that defines standards of care, and an independent evaluation team that judges quality and performance.
The pilot network was officially launched in September 2016, when all the partner organisations signed cooperation agreements covering issues relating to governance, cancer management teams, quality evaluation, and information sharing. The four core members include the Masaryk Memorial Cancer Institute in Brno – certified by the Organisation of European Cancer Institutes and by the US Joint Commission International; the Jihlava Cancer Centre, in the capital city of the Vysočina region; the University Hospital Brno, which specialises in haemato-oncology and childhood cancers; and St Ann’s University Hospital, Brno.
The first step was to change the data protection laws to allow the centralised sharing of data between hospitals and registries
Four general hospitals in the Vysočina region that treat patients with cancer are also part of the network, allowing multiple entry points, and helping ensure patients can undergo as much of their care as close to home as possible. The CCCN is also closely associated with the Masaryk University medical school, cancer research teams, tissue banks and bioinformatics facilities. All partners in the CCCN use standardised guidelines and referral pathways to help ensure uniformly high levels of care across the network.
Common cancers continue to be treated at all partner institutions as before, but that treatment now has to be in line with agreed protocols. This is what Luzzatto regards as the essential basis of a CCCN: “The main principle… is that patients are treated according to fully unified protocols. It doesn’t matter whether a patient goes to hospital A, B or C – wherever a patient comes in, he or she gets treated at that hospital according to the same high quality protocol.” This did not happen prior to the establishment of the network, says Dušek.
One caveat is surgery, where Luzzatto insists that, for particularly tricky operations, the patient must be referred to the best place in the network, even if their chemotherapy and radiotherapy is delivered nearer home.
Referral to specialist centres is also mandatory for any patient presenting with childhood cancers or haematological malignancies, who are all managed by specialist teams at Brno University Hospital.
Management of all patients with other rare cancers is concentrated at the Masaryk Memorial Cancer Institute.
By linking cancer centres, regional hospitals, primary care services and many other providers of services along the cancer care pathway, comprehensive cancer care networks are designed to ensure all aspects of a patient’s care are managed to uniformly high standards and protocols, as close to home as can safely be achieved, with clear pathways of referral between the different parts of the network. A network should be responsible for providing comprehensive cancer care to the entire population within its catchment area. Responsibility for planning and delivering all aspects of a patient’s care is in the hands of inter-professional, multidisciplinary, tumour-specific tumour management groups within the CCCN.
For Dušek, a data analyst, setting up a common information system has to be the first step in efforts to develop a CCCN, “because we need comprehensive and representative data on patient flow and patient presence in the region where you would like to change the structure of care. Without such data, you cannot convince stakeholders, you cannot convince politicians to do anything. And you need data to generate economic predictions.”
Customised software was developed early in the pilot and installed at every hospital in the network to enable common data sets to be gathered in a uniform way, for benchmarking and to facilitate tracking and analysis of transfer of patients among participant hospitals, survival outcomes and volume of care.
Much of this data on the pilot region, together with some analytic tools, are publicly available on the onconet.cz portal, which Dušek refers to as a “backbone of the eHealth system” in the Czech Republic. The portal aims to offer a ‘one-stop shop’ for patients and relatives seeking information on cancer care in their region, including details of how to contact the CCCN and individual contact details for the helpdesk of each tumour management group.
A pilot CCCN for Poland
Planning has begun for piloting a comprehensive cancer care network in Lower Silesia, a Polish province that borders on Germany and the Czech Republic. The pilot will be developed within the framework of the iPAAC European Joint Action on Cancer, which is taking forward the work started during the previous ‒ CanCon ‒ Joint Action.
The network will be centred around the Lower Silesian Oncology Centre, a comprehensive cancer centre that was established in the provincial capital Wroclaw in 1954. After several expansions, a new hospital with 600 beds is planned for 2023.
The Lower Silesian Oncology Centre, directed by Professor Adam Maciejczyk, is currently the only hospital in the region that offers all oncology treatment modalities. It caters not just for the inhabitants of Lower Silesia, but for people in the surrounding regions ‒ about 10 million in all.
Two branches of the Lower Silesian Oncology Centre, in Legnica and Jelenia Gora 70‒100km from Wroclaw, give patients who live further away access to radiotherapy.
The plans for developing a comprehensive cancer care network in the region are still at an early stage. Dorota Dudek-Godeau, one of the coordinators of the project, who is based at the National Institute of Public Health-National Institute of Hygiene in Warsaw, says a review of options was scheduled for an iPAAC meeting in February 2019, and would take reviews of the literature and results of surveys as the starting point.
Decisions on which units will join the network have yet to be finalised, she says, but regional hospitals have already indicated an interest in joining.
Unlike the networks being implemented in the Czech Republic, says Dudek-Godeau, this initiative is not being driven by national policy. The hope is that successfully planning, implementing and demonstrating the value of the Lower Silesia cancer care network, as part of the iPAAC project, could offer some solutions and recommendations for the National Cancer Network, the concept of which is currently being worked on by the Polish Ministry of Health.
An adaptable blueprint
A key element of the iPAAC Joint Action will focus on developing a generic model for setting up CCCNs that could apply in every national setting, and could be adapted by member states to fit their specific legal framework and health systems. The pilot study will also develop tumour-specific service guidelines, to ensure that patients are treated with identical diagnostics and treatment protocols regardless of which hospital they present at, with a particular focus on management of colorectal and pancreatic cancer. The same work package of iPAAC will develop models for how to derive quality indicators, implement patient-reported experience and outcomes measures (PROMs and PREMs), as well as create and implement patient pathways. These models will also be used in the Lower Silesian CCCN.
From competitors to partners
Dušek describes the establishment of the pilot CCCN as “a step-by-step transformation from the position of what I would call random assembly of hospitals to a well-organised and internally collaborating and communicating structure.”
But as Luzzatto admits, even if you know the steps to take, instituting change in complex systems that have set ways of doing things and are beset with vested interests can be a challenge.
“At the beginning, there can be friction,” he says, “but in the spirit of the CCCN, the participants must work together. Once the resistance is overcome, cooperation between major centres and smaller hospitals tends to work very well.”
“Of course, there are political issues,” he adds. “Comprehensive cancer centres are not always happy about CCCNs. In big cancer centres there may be big egos; sometimes they may look down on smaller centres. The pride of a comprehensive cancer centre is, justifiably, having a big institute with lots of patients, and a world-class research centre with up-to-date, expensive equipment within the same building or in the building next door. Of course, it is an advantage to have these under one roof… but this tends to empty other places of research.
“In my view, all those who are interested and capable, in whatever unit of a CCCN they find themselves, should be encouraged to take part in research. Otherwise, you create a ‘colonial situation’ in which the major centre uses others as satellites without involving them in the interesting stuff.”
“All those who are interested and capable, in whatever unit of a CCCN they are in, should be encouraged to take part in research”
By the same token, involving all the partners in developing the common treatment protocols is also important. “We shouldn’t belittle the peripheral hospitals.” Cooperating in research and treatment also has the added benefit of increasing the numbers of patients eligible for clinical trials.”
Do CCCNs improve outcomes?
As the Czech pilot CCCN has only been up and running for around two years, there is not yet enough evidence to attribute any improved survival to the changes in cancer care. What we do know, however, is that the way cancer patients are cared for has changed, says Dušek. “Results are very preliminary, but we very dramatically changed access to high-level, highly specialised cancer care for all citizens in the region, especially in Vysočina.
“Prior to the CCCN, only around 50% of cancer patients contacted cancer centres in their region; the rest were treated in general hospitals with some competing strategy.” Once the network was up and running, he says, “more than 80% were treated in touch points of the network and consulted primarily in tumour management teams, and haematological malignancies were transferred to Brno city.”
At least in the Czech Republic, the CCCN model seems likely to transform cancer care beyond the pilot region. “Of course, we would like to continue in improving the CCCN established in the pilot region,” said Dušek, “but the results are so convincing that we convinced … our minister of health, to export this model to the other regions of the country… The political leaders of healthcare accepted our strategy to distribute the CCCN model as an offered – not obligatory – model of cancer care in our country.”
More pilots planned
But the CCCN model may also have an impact beyond the borders of the Czech Republic. While the CanCon Joint Action ended in 2017, its successor, iPAAC (Innovative Partnership for Action Against Cancer, 2018–2021), includes a project to design a roadmap for implementing actions for cancer control.
Led by Simone Wesselmann, of the German Cancer Society (Deutsche Krebsgesellschaft), this work focuses on governance of integrated and comprehensive cancer care, and will include developing a framework for implementing and monitoring CCCNs.
“More than 80% of patients were treated in touch points of the network
and consulted primarily in tumour management teams”
Wesselmann sees this as an opportunity to help ensure the CCCN work done by CanCon translates into improved care and outcomes across Europe. “I think this is a great and important opportunity to deepen what was achieved in CanCon and ensure that the results aren’t lost but instead implemented.”
Two new CCCNs, one in Berlin, Germany, and one in lower Silesia, Poland (see box “A pilot CCCN for Poland”), will be implemented and audited as a pilot, she says.