Obesity is overtaking tobacco as the leading preventable cause of cancer. Oncologists have an important role to play in informing patients and directing them towards assistance in making lifestyle changes. Antonio Di Meglio reviews the links between obesity and cancer, the implications of weight gain after diagnosis and treatment, and strategies to help patients lower their weight-related risk.
This grandround was first presented by Antonio Di Meglio, from the Gustave Roussy Institute, Villejuif, France, as a live webcast for the European School of Oncology. It was edited by Susan Mayor. The webcast of this and other e-sessions can be accessed at e-eso.net.
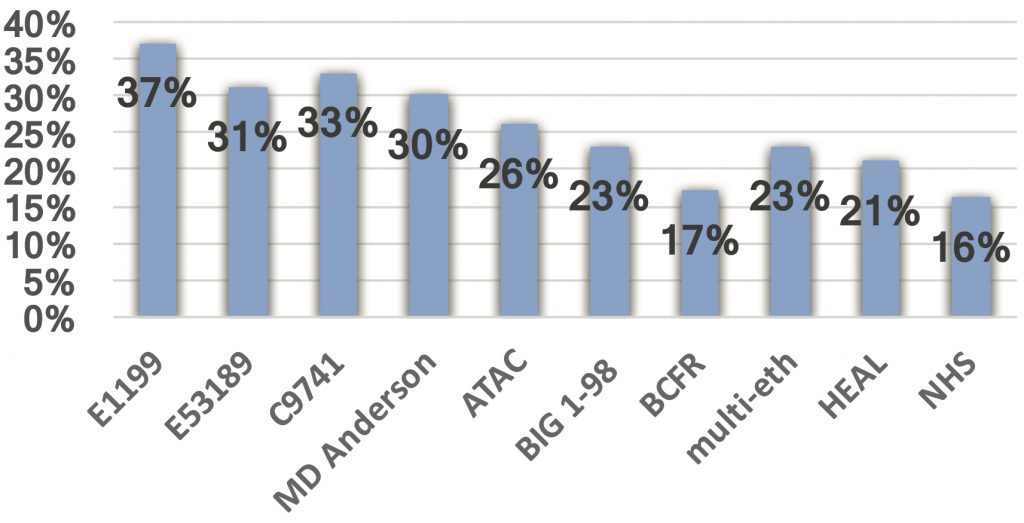
Obesity has a major impact on cancer. The proportion of cancers attributable to obesity is increasing so much that obesity is now overtaking tobacco as the leading preventable cause of cancer, with recent figures from the US showing that it accounts for 4% of cancers in men and 7% of cancers in women (Cancer Detect Prev 2008, 32:190–199; Lancet 2011, 378:815–25). Several studies have shown high rates of obesity in cancer patients at the point of diagnosis, as defined by a body mass index (BMI) of 30 kg/m2 and higher. For example, the French national CANTO cohort, which included more than 12,000 patients diagnosed with early breast cancer between 2012 and 2018, showed that the prevalence of obesity at the time of diagnosis was 19.2%, and this increased to 20.3% at one year after diagnosis and to 20.9% at two years (Ann Oncol 2018, 29 Suppl 8).
The link between obesity and cancer
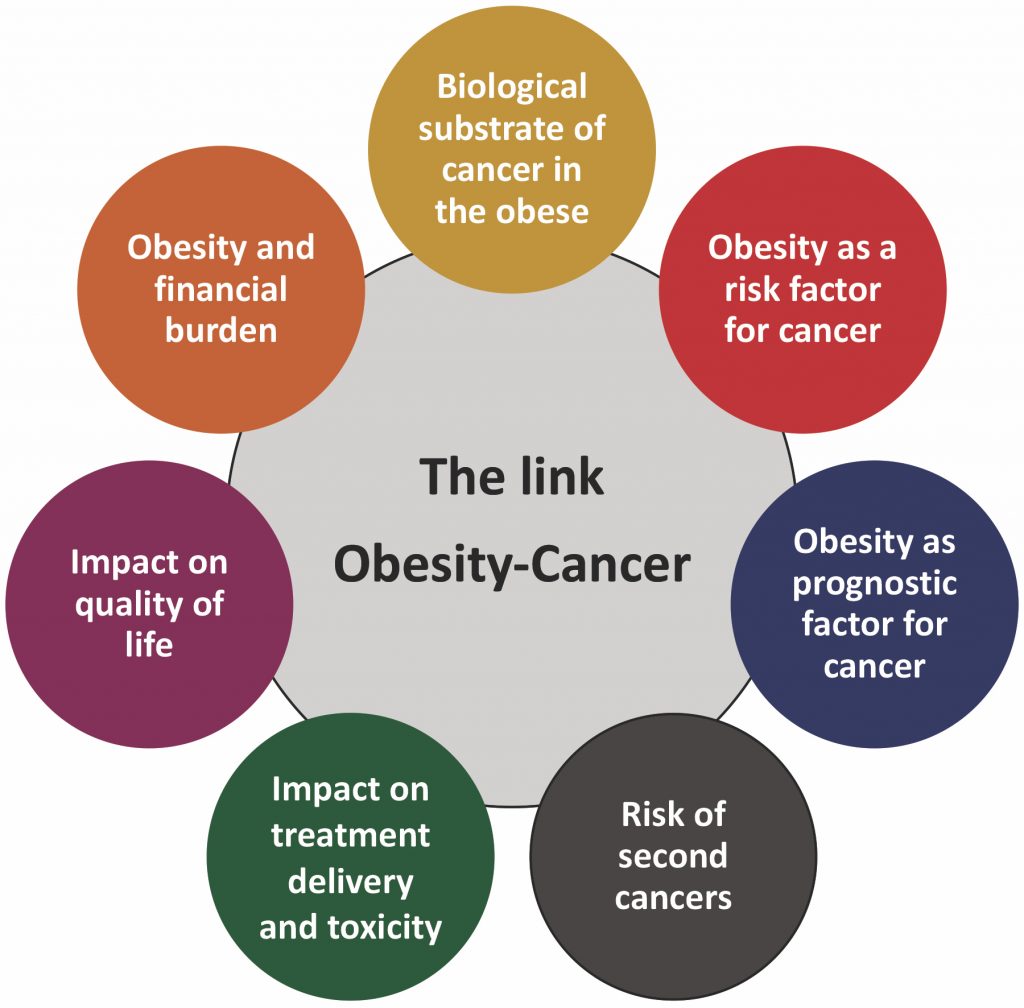
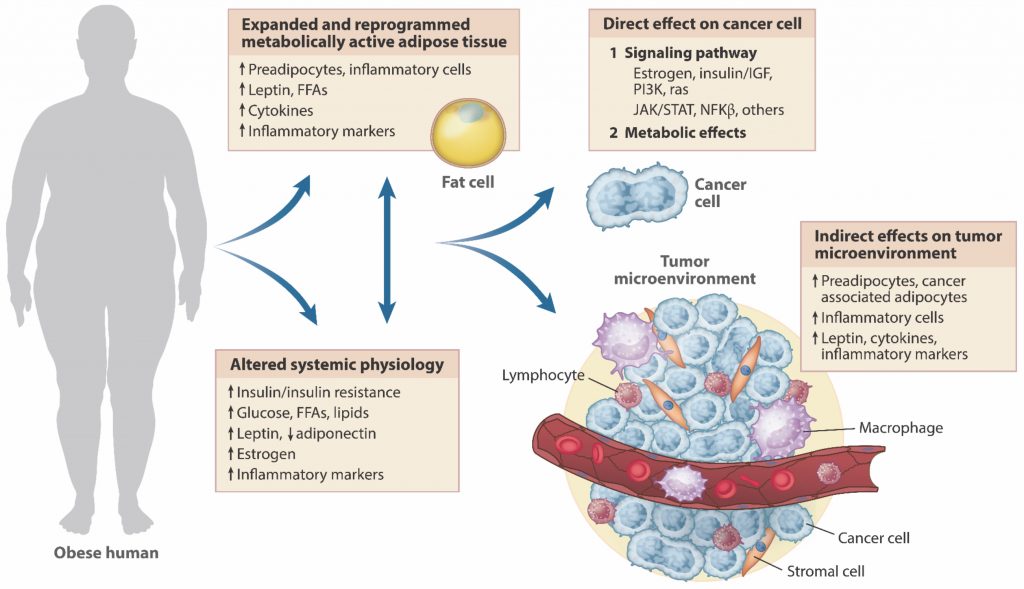
There are many aspects to consider in the link between obesity and cancer. The first relates to the biological substrate of cancer in obese individuals. People who are obese have expanded and reprogrammed metabolically active adipose tissue with an increase in several mediators, including pre-adipocytes, inflammatory cells, cytokines and other inflammatory markers. The adipose tissue interacts with an altered systemic physiology, with an increase in circulating levels of insulin and glucose. This interplay has a direct impact on cancer cells, through enhancing signalling pathways in addition to a direct metabolic effect. In addition, the interplay has also many indirect effects on the tumour microenvironment (see figure “Underlying biological mechanisms”).
Prevalence of obesity at diagnosis in breast cancer patients across studies
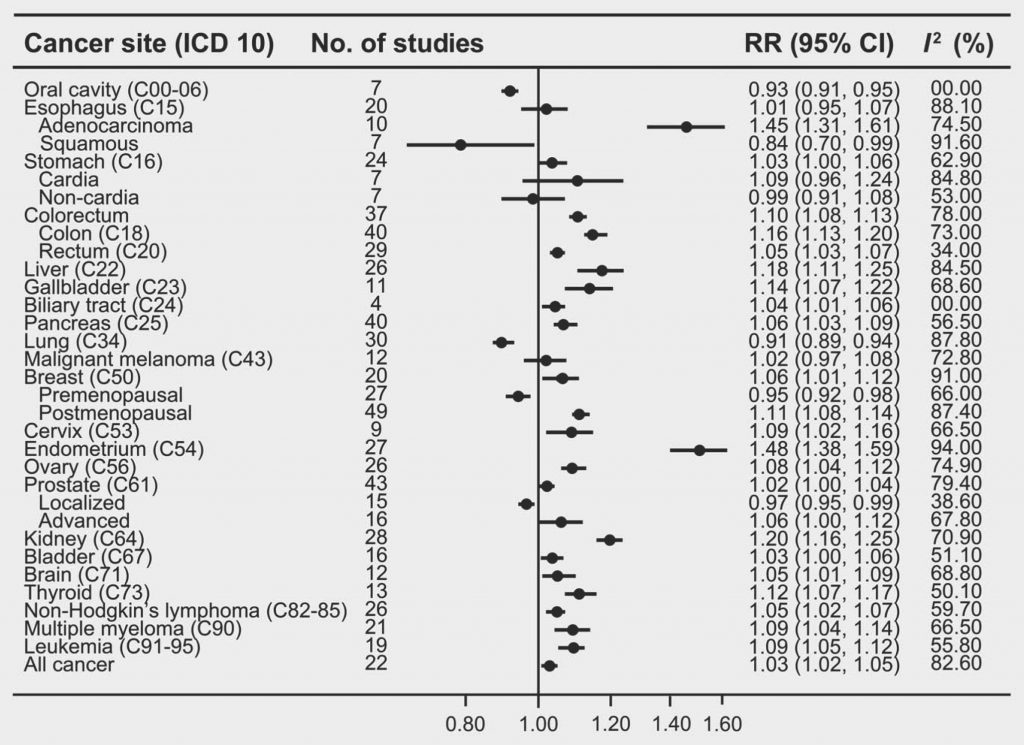
Second, obesity is an established risk factor for cancer. A recent analysis (Int J Cancer 2018, 143:1595–603) showed a strong positive association between BMI and several types of cancer, including endometrial cancer, oesophageal adenocarcinoma, postmenopausal breast cancer and kidney cancer (see figure “Multiple studies show an association between obesity and cancer”).
In contrast, there seemed to be an inverse relationship between BMI and risk of oral cavity cancer, lung cancer and premenopausal breast cancer. The relationship between obesity and cancer is also sex specific, with a higher risk of colorectal cancer among obese males and increased risk of brain and kidney cancer among obese females.
Third, obesity is also a prognostic factor for many cancers. Data linking obesity to poor outcomes are strongest in breast, colorectal and prostate cancer. There is also compelling evidence starting to emerge for other cancers, including childhood leukaemia.
There are mixed data on obesity in colon cancer. Some studies have shown that very obese patients (BMI>35 kg/m2) have increased risk of colon cancer recurrence, total mortality and colon cancer-related mortality (JNCI 2006, 98:1647–54). However, a meta-analysis of adjuvant chemotherapy trials in colon cancer found that the association between increased BMI and poorer outcomes was sex specific (Cancer 2013, 119:1528–36), with a significant prognostic effect of BMI in men for both disease-free and overall survival, but not in women.
There is also evidence that patients with prostate cancer who are obese may have poorer outcomes, and that obesity is associated with the development of more biologically aggressive and more advanced prostate cancer (Cancer Epidemiol Biomarkers Prev 2006, 15:1977–83).
Finally, a study in children and adolescents with acute lymphoblastic leukaemia has shown obese patients had worse outcomes than those who were not obese (JCO 2007, 25:2063–69).
Fourth, obesity increases the risk of second cancers. Together with other modifiable lifestyle factors, obesity has been shown to be associated with a higher risk of a second primary breast cancer. One study demonstrated a 40% higher risk of developing contralateral breast cancer in women who were obese at diagnosis of oestrogen-receptor positive breast cancer (JCO 2009, 27:5312–18).
In another study, which accounted for use of screening, access to treatment, type of treatment, use of adjuvant therapy, and tumour characteristics, there was a more than two-fold increased risk of recurrence among obese patients compared with normal-weight patients with breast cancer (Cancer Causes Control 2013, 24:305–12).
Impact on cancer diagnosis and treatment
Another way that obesity impacts cancer is through its effect on diagnosis and the delivery of treatment and its toxicity in cancer patients. Obese individuals may delay seeking medical care and may be less likely than the non-obese to participate in screening programmes (J Gen Intern Med 2009, 24:665–77; J Obesity 2011, doi:10.1155/2011/218250). The accuracy of diagnostics may also be reduced in obese patients, as shown in studies reporting haemodilution of tumour biomarkers and impaired quality of imaging among obese cancer patients (J Urol 2009, 181:567–73; Crit Rev Oncol Hematol 2013, 85:193–205).
In terms of treatment, there can be technical difficulties in the delivery of radiation therapy and surgical management in obese patients (Radiother Oncol 2009, 91:114–19).
In addition, studies have shown higher rates of thromboembolism in obese patients receiving chemotherapy (JCO 2006, 24:484–90), and a study in patients undergoing major abdominal cancer surgery found that higher BMI was associated with increased rates of post-surgical complications and wound infections (Ann Surg Oncol 2008, 15:2164–72).
Implications of weight gain after cancer diagnosis and treatment
Weight gain after cancer is another very important problem. Many cancer survivors gain weight after being diagnosed with cancer, particularly those treated with chemotherapy and women who transition to post-menopausal status as a result of cancer treatment.
On average these patients gain 2–5 kg, but weight gain can be as high as 10 kg in the first two years after cancer diagnosis.
Sarcopenic obesity is also particularly common in cancer patients, consisting in loss of muscle mass and concomitant gain of adipose tissue. It can occur in patients treated with chemotherapy, but also with androgen deprivation therapy for prostate cancer.
In an analysis using data from the French national CANTO cohort, among more than 4,500 patients with early breast cancer diagnosed between 2012 and 2015, one in four gained substantial weight (at least 5% of baseline weight) two years after diagnosis, with an average increase of 6–7 kg (Front Onc 2018, 29 Suppl 8:620–21).
Many factors were associated with a higher likelihood of gaining weight by two years post-diagnosis, including treatment with chemotherapy, younger age at diagnosis, lower physical activity levels and gaining weight within one year following diagnosis.
The link between obesity and cancer
Weight gain after being diagnosed with breast cancer may be associated worse breast cancer outcomes, but studies have shown inconsistent results. A higher risk of breast cancer recurrence among women who gained more than 2.0 kg/m2 after diagnosis was reported (JCO 2005, 23:1370–78), although other studies showed similar rates of breast cancer recurrence among women who gained weight and those who maintained their baseline weight (Breast Cancer Res Treat 2006, 99:47–57).
Obesity and post-diagnosis weight changes also have important implications in terms of quality of life of cancer patients.
An analysis of obese patients with early breast cancer among the CANTO cohort showed that gaining at least 5% of baseline weight between diagnosis and completion of primary treatment was associated with the highest rates of severely impaired patient-reported functions and worse symptoms. Conversely, losing at least 5% of baseline weight was associated with a significantly reduced risk of severe dysfunction or reduced quality of life at one year after diagnosis (Ann Onc 2018, 29 Suppl 8:620–21).
Strategies to promote weight loss or prevent weight gain in cancer survivors
There is now increased awareness of the availability and benefit of strategies to promote weight loss or prevent weight gain in cancer survivors. Studies with these strategies, and particularly those that include calorie restriction, increased physical activity and behavioural counselling, have consistently demonstrated that weight loss of 5–7% of body weight may reduce the incidence of other diseases, particularly diabetes and cardiovascular disease, and improve several general and cancer-specific outcomes.
ASCO published a key position statement on obesity and cancer a few years ago (JCO 2014, 32:3568–74). It has also released a guide for oncology providers on obesity and cancer that provides guidance on selecting weight loss treatments for cancer survivors (bit.ly/ASCO_Obesity-Cancer).
Underlying biological mechanisms
FFA – free fatty acids, IGF –insulin-like growth factor Source: PJ Goodwin and V Stambolic (2015) Annu Rev Med 66:281–296. Reproduced with permission of Annual Reviews
People who are obese have expanded and reprogrammed metabolically active adipose tissue with an increase in several mediators for cancer
According to this guide, the use of lifestyle therapy based on diet, physical activity and behavioural therapy should be recommended to support weight loss in all cancer survivors who have a BMI that is greater than 30 kg/m2, as well as in those whose BMI is between 25 and 30 kg/m2, if they suffer from two or more comorbidities.
Further strategies to facilitate weight loss are also reviewed in this ASCO guide, including pharmacotherapy for patients who have not lost 1 lb (0.45 kg) per week after six months of lifestyle therapy, and bariatric surgery only in selected patients who particularly struggle to lose weight. Lifestyle strategies for prevention of further weight gain are always indicated in any patient with a BMI of more than 25 kg/m2.
Lifestyle interventions to facilitate weight loss have been tested in multiple settings in oncology care.
The Lifestyle Intervention Study for Adjuvant Treatment of Early Breast Cancer (LISA) is the largest weight loss intervention study in cancer (JCO 2014, 32:2231–39). It included breast cancer patients treated with adjuvant letrozole and with a BMI>24 kg/m2. They were randomised to a control arm or a two-year telephone-based intervention with individualised goals of 10% weight loss, a calorie restriction of 500–1,000 fewer calories per day, and 150–200 minutes of moderate-intensity physical activity per week. Even though accrual to the trial was interrupted because of funding issues, results showed significantly greater mean weight loss among patients in the intervention group compared to the control group (-3.1 kg vs -0.3 kg at two years).
Another trial, the Active After Cancer Trial (AACT), in survivors of breast and colorectal cancer who were not physically active at the time of diagnosis, showed that a 16-week telephone-based exercise intervention improved physical performance and physical functioning compared to a control arm (Breast Cancer Res Treat 2012, 132:205–13). This study also confirmed the feasibility of using cooperative clinical trials systems for conducting lifestyle interventional research.
Lifestyle interventions are now deemed to be safe and feasible in cancer populations, and several studies have shown benefits in different types of cancer. Results have shown a positive impact on quality of life and favourable changes in cancer biomarkers. Lifestyle interventions also hold the promise to improve cancer outcomes, but this is still an open question that ongoing trials are trying to address. One such trial is the Breast Cancer Weight Loss (BWEL) study (NPJ Breast Cancer 2017, 3:37), which is randomising 3,136 participants with a BMI of 27 kg/m2 or higher to two arms: a health education control arm versus health education plus two years of supervised weight loss programme based on caloric restriction and increased physical activity, delivered remotely by a personalised lifestyle coach. The primary endpoint of BWEL is evaluating the impact of weight loss on breast cancer invasive-disease-free survival.
Multiple studies show an association between obesity and cancer
RR– relative risk Source: J Min, F Wang, S Liu et al. (2018) Int J Cancer 143:1595-603. Republished with permission from John Wiley and Sons
A systematic review and quantitative meta‐analysis of cohort studies reporting body mass index (BMI) and the risk of 23 cancer types revealed the following associations:
Positive association of increasing BMI with cancers occurring in a wide range of sites.
Strong positive associations between BMI and
endometrial cancer (RR: 1.48)
oesophageal adenocarcinoma (RR: 1.45)
postmenopausal breast cancer (RR: 1.11)
kidney cancer (RR: 1.20);
Signi cant inverse associations between BMI and
oral cavity cancer (RR: 0.93)
lung cancer (RR: 0.91)
premenopausal breast cancer (RR: 0.95)
localised prostate cancer (RR: 0.97)
A male-speci c association between BMI and
colorectal cancer
A female-speci c association between BMI and
brain cancer
kidney cancer
In addition, one of the important questions that we should ask ourselves when conducting research testing lifestyle interventions in cancer survivors, and also in analysing the impact of obesity on cancer, is whether cancer survivors behave differently to the general population. Research suggests they are no more likely to engage in healthy behaviours, including regular physical activity or consuming at least five servings of fruit or vegetables per day, than adults without a history of cancer (Cancer Prev Res (Phila) 2011, 4:522–29; JCO 2008, 26:3958–64; Cancer Epidemiol Biomarkers Prev 2009, 18:87–95; JAMA 2005, 293:2479–86).
Overall, studies have shown that the prevalence of inactive patients among cancer survivors is very high.
ASCO guidelines on weight management and physical activity
Nevertheless, cancer organisations such as ASCO are working to raise awareness about the importance of cancer as a ‘teachable moment’ for patients. This views cancer as “a naturally occurring life transition or health event that has the potential to motivate individuals to adopt risk-reducing or health protecting behaviours” (JCO 2005, 23:5814–30).
Several studies support the notion that most cancer survivors are interested in health promotion programmes, with a preference for home-based formats. Many cancer survivors report dietary changes or stopping smoking after being diagnosed with cancer.
However, there are barriers and limitations to using cancer as a teachable moment. Factors reducing the likelihood of healthy lifestyle adoption include: male sex and older age, lower education, or living in urban areas.
Physicians, and particularly oncologists, can make a real difference because they are the most powerful catalysts for promoting behavioural change in cancer patients. Nevertheless, a study showed that only 20% of oncology care physicians provided assistance for lifestyle changes (JCO 2005, 23:5814–30), because of competing concerns, uncertainty regarding the type and most appropriate health behaviour messages to give, and issues regarding insurance coverage and reimbursement of lifestyle interventions. The ASCO obesity initiative is trying to address these concerns.
The ASCO Position Statement on Obesity and Cancer (JCO 2014, 32:3568–74) proposes a practical approach to weight management in cancer patients and survivors based on assessment of BMI, giving advice and referring to local resources. First, physicians should always assess BMI, as a simple measure that does not require any special equipment. Second, health professionals should advise patients on weight management in a neutral manner, including BMI as part of reviews and discussing exercise habits and weight issues. Particularly, it is important to acknowledge the challenges and struggles that patients may face in trying to lose weight. Finally, it is crucial to identify local resources, particularly dieticians and nutritionists, who have specific training in the oncology setting and can provide tailored support for individual patients.
There are also guidelines from the American College of Sports Medicine that provide guidance to cancer survivors on physical activity (Med Sci Sports Exerc 2010, 42:1409–26). They suggest that adults aged 18 to 64 should engage in at least 150 minutes of moderate-intensity physical activity per week, or 75 minutes of vigorous physical activity per week, or an equivalent combination. Moderate activities include biking on level ground, general gardening, tennis or walking briskly, while vigorous activities include fast cycling, hiking uphill, race walking or jogging and fast swimming or swimming laps.
Summing up
Obesity has reached epidemic levels worldwide, with more than one in three adults in the US categorised as obese, and these figures are very consistent in the rest of the Western world. Obesity is now becoming the leading preventable cause of cancer, with a prevalence of up to 40% in cancer patients.
There is a strong link between obesity and cancer, and compelling evidence exists that obesity acts as a risk factor and prognostic factor in cancer and that it can negatively impact treatment toxicity and quality of life and pose an important financial burden in cancer care.
There is also a major problem with weight gain after cancer, with a substantial proportion of patients gaining weight after their cancer diagnosis and treatment.
In the contemporary scenario of cancer survivorship, it is essential that weight control and weight loss strategies based on lifestyle interventions become part of standard oncology care.




This grandround was first presented by Antonio Di Meglio, from the Gustave Roussy Institute, Villejuif, France, as a live webcast for the European School of Oncology. It was edited by Susan Mayor. The webcast of this and other e-sessions can be accessed at e-eso.net.