Cancer is not the first thing that springs to mind when one thinks about conflict and refugees, but bear with me and I will explain why this is such a problem now. Back in the 2000’s I was involved with a European Investment Bank initiative to fund, build and resource two new cancer centres in Syria; one in Aleppo and one in Homs, which respectively saw 36% and 14% of all cancer referrals. Despite being a demographically young country, 73% of avoidable mortality in Syria was due to non-communicable diseases (NCDs).
Syria had not only fully transitioned from a low- to a middle-income country, but it was also host to an influx of refugees from Iraq, and by July 2007 it hosted some 1.4 million, which was increasing at a rate of 30,000 per month.
Outside some stable urban centres, cancer control and care has now ostensibly been wiped out across Syria. With an estimated two thirds of healthcare professionals now refugees (see www.sams-usa.net/foundation/), rebuilding any sort of ‘national’ cancer control system will take a generation, or more.
Across the Middle East and Africa, protracted armed conflicts, some now lasting more than a decade, are having dramatic effects on migration. By the end of 2014 the UN estimated that there were some 19.5 million refugees, of which 2.9 million were not under UN protection. Internal displacement had also reached nearly 40 million.
What has been so different over the last decade is that this is happening to demographically transitioned countries like Iraq, Syria and Libya, with ageing populations and high burdens of cancer prior to the outbreak of conflicts. In many cases these countries had reasonably developed levels of cancer care.
The new humanitarian space is one in which NCD control and management is now absolutely necessary. The problem is that humanitarian models of care have developed around delivering acute care for infectious diseases, trauma and maternal and child health.
Cancer is a completely new care paradigm for the likes of Médicins sans frontières and the Red Cross. Less obvious impacts of conflict include the likes of Palestine, where isolation and counter insurgency tactics have meant little infrastructure and expertise is available for treating cancer (Med Confl Surviv 2014, 30:4–10). A blogpost by Shayma al-Waheidi about the challenge of improving breast cancer outcomes in Gaza gives one some idea of what this means for the average cancer patient (thecancerblog.net/closing-the-40-survival-gap-in-gaza). Even non-traditional conflicts, such as the drug wars in Latin America, have reduced access to cancer care in some regions of Mexico to almost zero, as healthcare professionals have left.
Good cancer care requires all the attributes of a functioning healthcare system, and these are exquisitely sensitive to conflict. But the nature of today’s conflicts – protracted duration, intrastate, fought by irregular armed groups, and fuelled by economic opportunities and ethnic rivalry – have created an even more toxic environment for any sort of cancer care during the conflict or in the long tail of the post-conflict period (Lancet 2010, 375:341–345).
Prevention policies for cancer and other NCDs also dramatically suffer. Smoking prevalence, for example, has jumped to over one third of the population in Iraq, with a parallel collapse in governance and legislation around anti-tobacco measures. The UN Refugee Agency, UNHCR, has continued to struggle with the burden of cancer in refugee camps under its care.
Health services for refugees are nominally capped at $1,000–$2,000 per person per year, which is far short of even the cheapest cancer treatment. Refugees diagnosed with cancer have to have their cases reviewed on a per patient basis by the UNHCR’s Exceptional Care Committees.
In Jordan, between 2010 and 2012, only 511 of the cases reviewed were for cancer (only a fraction of what would be projected to be diagnosed in the camps). Of these, breast, colorectal and soft tissue cancers made up the majority (44%), but only half were authorised for treatment, with poor prognosis a major cause of rejection (Lancet 2014, 15:e290–e297).
All the evidence points to a massive deficit in both funding and processes to address cancer within the UNHCR system. However, the impact on countries like Jordan, looking after both registered and unregistered refugees, is even more profound, placing a huge burden on an already overstretched cancer system. Institutions like the King Hussein Cancer Foundation have been left to support many refugees diagnosed with cancer through zakat (charitable) funds.
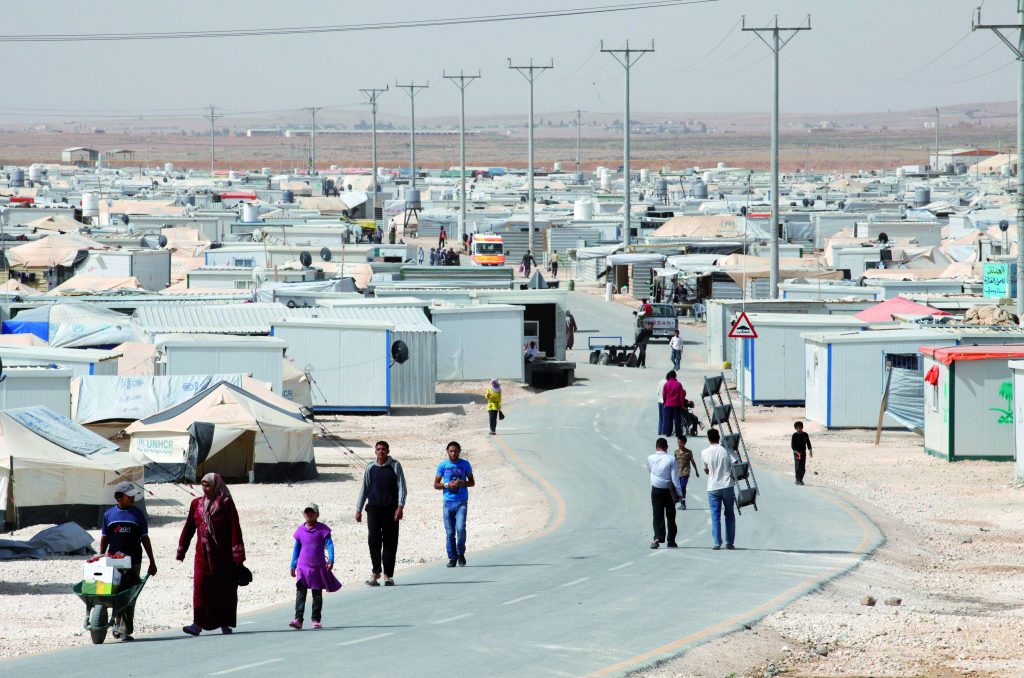
Old paradigms of camp-based refugee care, focusing only on infectious diseases, malnutrition and child-maternal health, are no longer sufficient
But this is clearly not a sustainable situation. Further afield, Tunisia is also feeling the impact of the collapse of security in Libya, with an estimated 2 million refugees, and as migration continues across Europe, more refugees will be diagnosed with cancer with no clear models of care in place.
Cancer policies and interventions have not kept up with the profound global changes in conflict settings in the last decade. Old paradigms of camp-based refugee care, focusing only on infectious diseases, malnutrition and child-maternal health, are no longer sufficient.
Tackling NCDs, and cancer in particular, is complicated and expensive relative to other areas. However, cancer enjoys substantial funding from both public and private sectors in high-income countries, and there is an ethical duty to help countries and organisations deliver and rebuild cancer control and care. This will require far better cancer intelligence in refugee settings, and the post-conflict environment, and new financing and referral models.
* Richard Sullivan is Director of the Institute of Cancer Policy
and Conflict and Health Programme at Kings Health Partners